

Modified Functional Reach Test: Upper-Body Kinematics and Muscular Activity in Chronic Stroke Survivors
- PMID: 35009772
- PMCID: PMC8749777
- DOI: 10.3390/s22010230
Modified Functional Reach Test: Upper-Body Kinematics and Muscular Activity in Chronic Stroke Survivors
Abstract
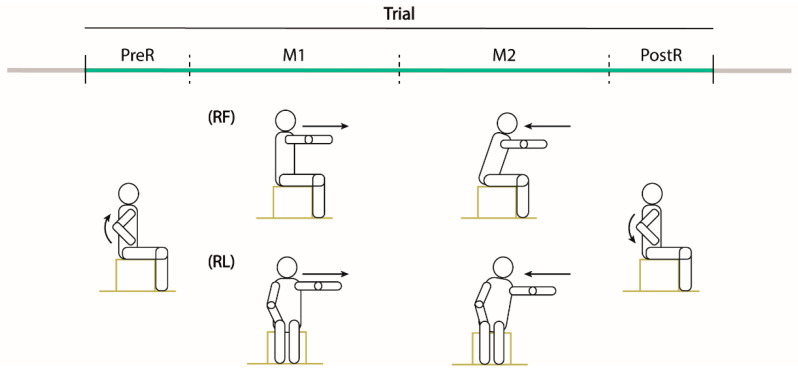
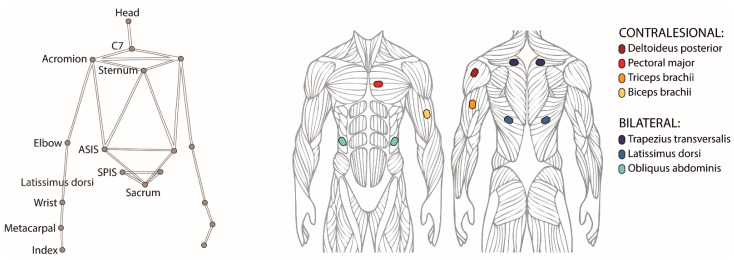
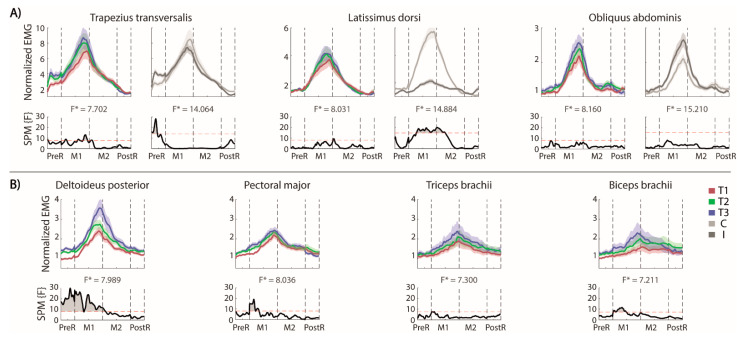
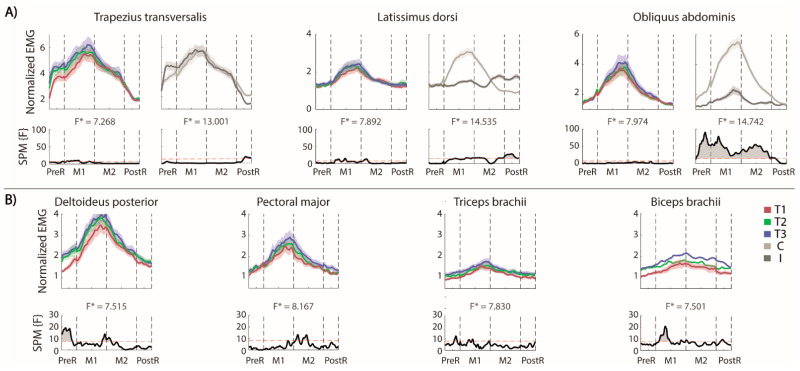
Effective control of trunk muscles is fundamental to perform most daily activities. Stroke affects this ability also when sitting, and the Modified Functional Reach Test is a simple clinical method to evaluate sitting balance. We characterize the upper body kinematics and muscular activity during this test. Fifteen chronic stroke survivors performed twice, in separate sessions, three repetitions of the test in forward and lateral directions with their ipsilesional arm. We focused our analysis on muscles of the trunk and of the contralesional, not moving, arm. The bilateral activations of latissimi dorsi, trapezii transversalis and oblique externus abdominis were left/right asymmetric, for both test directions, except for the obliquus externus abdominis in the frontal reaching. Stroke survivors had difficulty deactivating the contralesional muscles at the end of each trial, especially the trapezii trasversalis in the lateral direction. The contralesional, non-moving arm had muscular activations modulated according to the movement phases of the moving arm. Repeating the task led to better performance in terms of reaching distance, supported by an increased activation of the trunk muscles. The reaching distance correlated negatively with the time-up-and-go test score.
Keywords: MFRT; ipsilesional arm; sEMG; sitting balance; trunk control.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
