

Oxygen Imaging for Non-Invasive Metastasis Detection
- PMID: 35009780
- PMCID: PMC8749708
- DOI: 10.3390/s22010237
Oxygen Imaging for Non-Invasive Metastasis Detection
Abstract
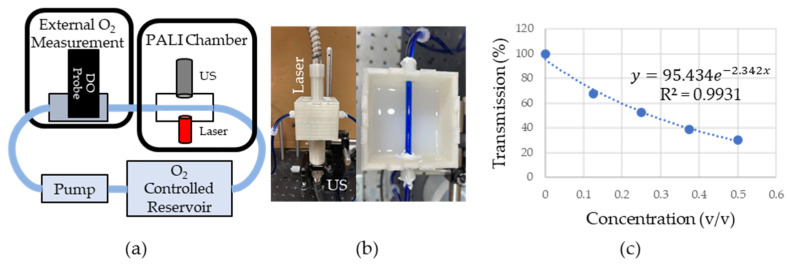
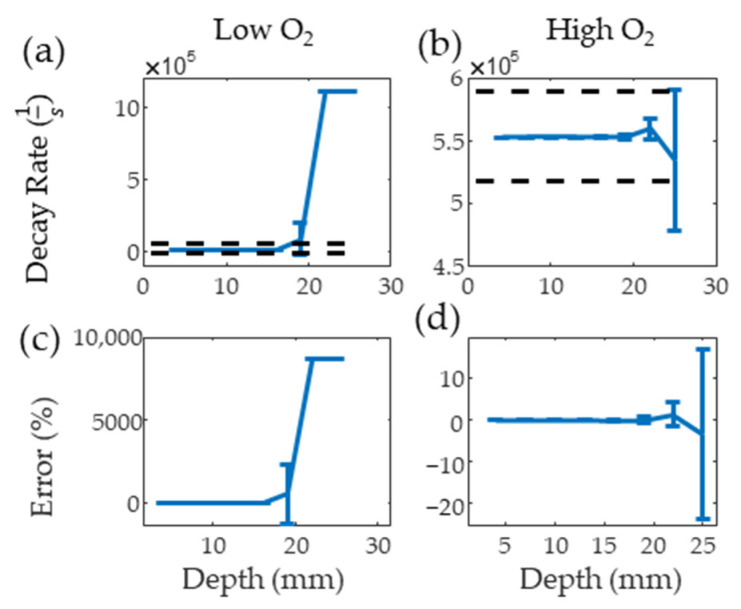
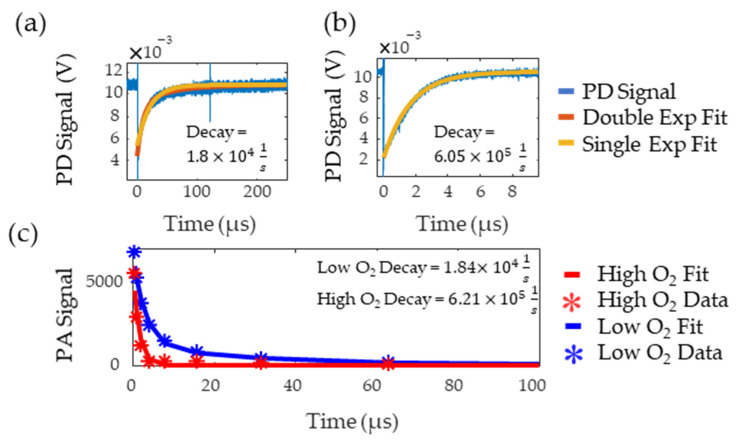
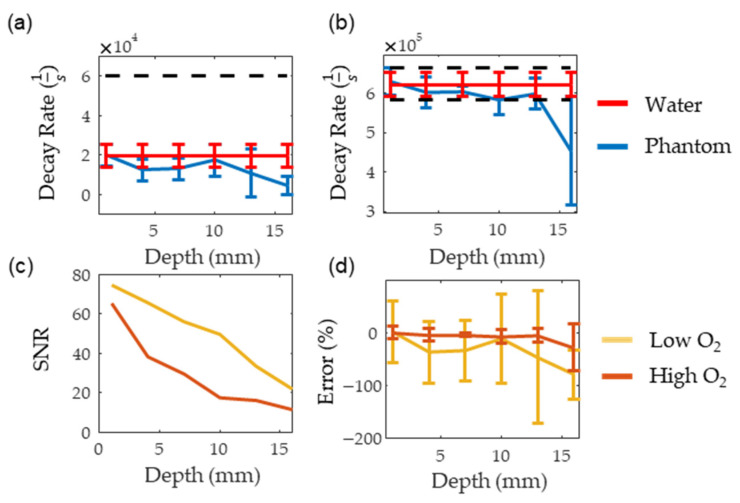
Sentinel lymph node (SLN) biopsy is an integral part of treatment planning for a variety of cancers as it evaluates whether a tumor has metastasized, an event that significantly reduces survival probability. However, this invasive procedure is associated with patient morbidity, and misses small metastatic deposits, resulting in the removal of additional nodes for tumors with high metastatic probability despite a negative SLN biopsy. To prevent this over-treatment and its associated morbidities for patients that were truly negative, we propose a tissue oxygen imaging method called Photoacoustic Lifetime Imaging (PALI) as an alternative or supplementary tool for SLN biopsy. As the hyper-metabolic state of cancer cells significantly depresses tissue oxygenation compared to normal tissue even for small metastatic deposits, we hypothesize that PALI can sensitively and specifically detect metastases. Before this hypothesis is tested, however, PALI's maximum imaging depth must be evaluated to determine the cancer types for which it is best suited. To evaluate imaging depth, we developed and simulated a phantom composed of tubing in a tissue-mimicking, optically scattering liquid. Our simulation and experimental results both show that PALI's maximum imaging depth is 16 mm. As most lymph nodes are deeper than 16 mm, ways to improve imaging depth, such as directly delivering light to the node using penetrating optical fibers, must be explored.
Keywords: head and neck cancer; imaging; oxygen imaging; photoacoustic; sentinel lymph node biopsy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Prediction of additional lymph node involvement in breast cancer patients with positive sentinel lymph nodes.Neoplasma. 2016;63(3):427-34. doi: 10.4149/312_150922N497. Neoplasma. 2016. PMID: 26925789
-
Prediction of Extracapsular Invasion at Metastatic Sentinel Nodes and Non-sentinel Lymph Nodal Metastases by FDG-PET in Cases with Breast Cancer.Anticancer Res. 2016 Apr;36(4):1785-9. Anticancer Res. 2016. PMID: 27069160
-
Sentinel lymphadenectomy without systematic axillary dissection in breast cancer patients: predictors of non-sentinel lymph node metastasis.Eur J Surg Oncol. 2003 May;29(4):403-6. doi: 10.1053/ejso.2002.1427. Eur J Surg Oncol. 2003. PMID: 12711299
-
FDG-PET for axillary lymph node staging in primary breast cancer.Eur J Nucl Med Mol Imaging. 2004 Jun;31 Suppl 1:S97-102. doi: 10.1007/s00259-004-1531-z. Epub 2004 May 5. Eur J Nucl Med Mol Imaging. 2004. PMID: 15133635 Review.
-
Sentinel lymph node mapping in breast cancer: a critical reappraisal of the internal mammary chain issue.Q J Nucl Med Mol Imaging. 2014 Jun;58(2):114-26. Q J Nucl Med Mol Imaging. 2014. PMID: 24835288 Review.
Cited by
-
Photoacoustic lifetime oxygen imaging of radiotherapy-induced tumor reoxygenation In Vivo.J Photochem Photobiol. 2024 Jun;21:100241. doi: 10.1016/j.jpap.2024.100241. Epub 2024 Apr 27. J Photochem Photobiol. 2024. PMID: 39005728 Free PMC article.
-
Personalized Oncology by In Vivo Chemical Imaging: Photoacoustic Mapping of Tumor Oxygen Predicts Radiotherapy Efficacy.ACS Nano. 2023 Mar 14;17(5):4396-4403. doi: 10.1021/acsnano.2c09502. Epub 2023 Feb 27. ACS Nano. 2023. PMID: 36847392 Free PMC article.
References
-
- Van den Brekel M.W.M., Castelijns J.A., Stel H.V., Golding R.P., Meyer C.J.L., Snow G.B. Modern imaging techniques and ultrasound-guided aspiration cytology for the assessment of neck node metastases: A prospective comparative study. Eur. Arch. Otorhinolaryngol. 1993;250:11–17. doi: 10.1007/BF00176941. - DOI - PubMed
-
- Yoon D.Y., Hwang H.S., Chang S.K., Rho Y.S., Ahn H.Y., Kim J.H., Lee I.J. CT, MR, US, 18F-FDG PET/CT, and their combined use for the assessment of cervical lymph node metastases in squamous cell carcinoma of the head and neck. Eur. Radiol. 2009;19:634–642. doi: 10.1007/s00330-008-1192-6. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
