

Iron Deficiency in Heart Failure: Mechanisms and Pathophysiology
- PMID: 35011874
- PMCID: PMC8745653
- DOI: 10.3390/jcm11010125
Iron Deficiency in Heart Failure: Mechanisms and Pathophysiology
Abstract
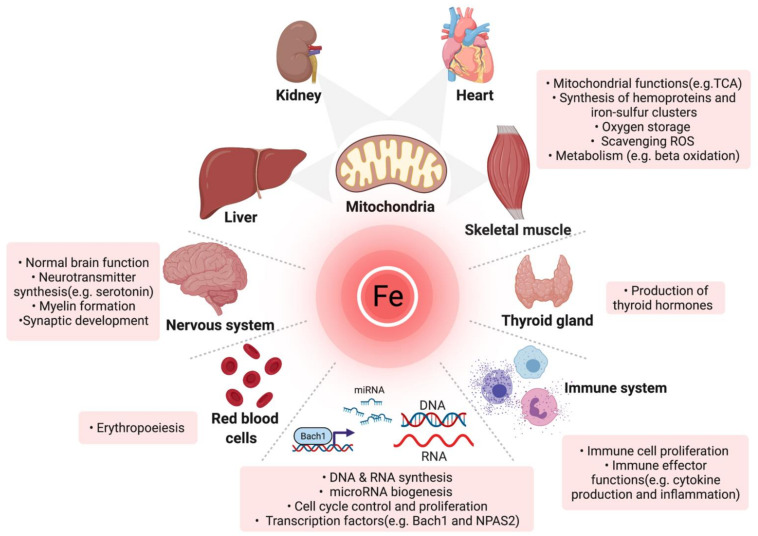
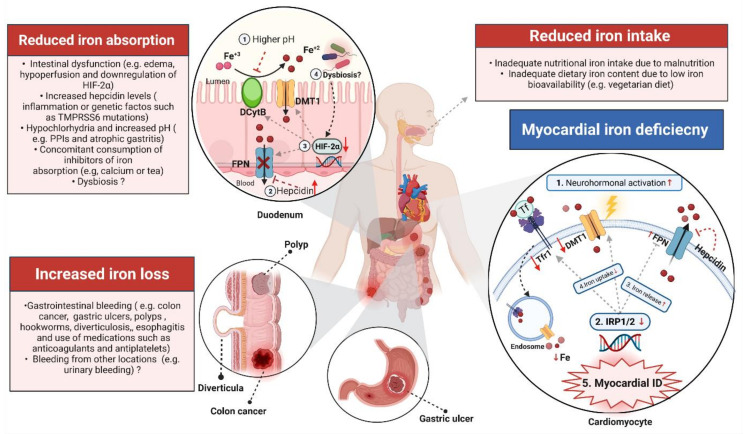
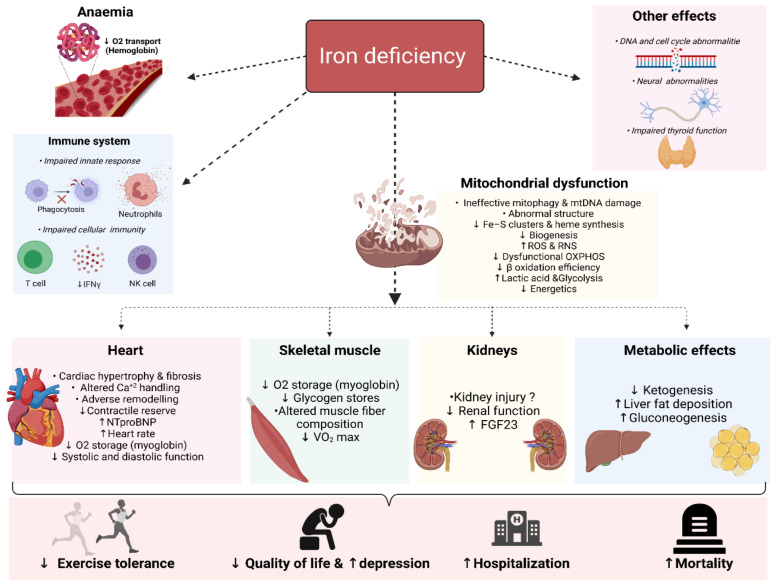
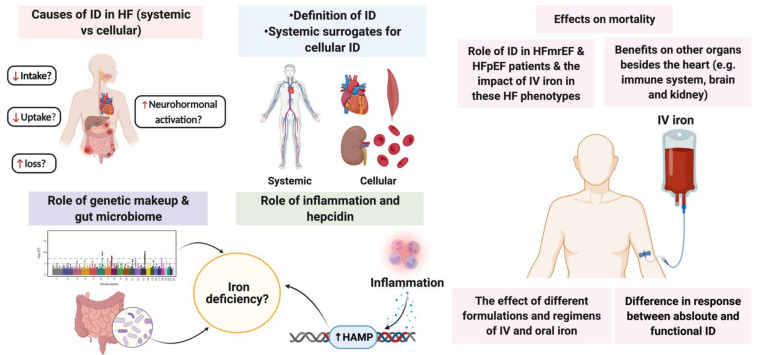
Iron is an essential micronutrient for a myriad of physiological processes in the body beyond erythropoiesis. Iron deficiency (ID) is a common comorbidity in patients with heart failure (HF), with a prevalence reaching up to 59% even in non-anaemic patients. ID impairs exercise capacity, reduces the quality of life, increases hospitalisation rate and mortality risk regardless of anaemia. Intravenously correcting ID has emerged as a promising treatment in HF as it has been shown to alleviate symptoms, improve quality of life and exercise capacity and reduce hospitalisations. However, the pathophysiology of ID in HF remains poorly characterised. Recognition of ID in HF triggered more research with the aim to explain how correcting ID improves HF status as well as the underlying causes of ID in the first place. In the past few years, significant progress has been made in understanding iron homeostasis by characterising the role of the iron-regulating hormone hepcidin, the effects of ID on skeletal and cardiac myocytes, kidneys and the immune system. In this review, we summarise the current knowledge and recent advances in the pathophysiology of ID in heart failure, the deleterious systemic and cellular consequences of ID.
Keywords: heart failure; iron deficiency; iron metabolism; pathophysiology.
Conflict of interest statement
The UMCG, which employs several of the authors, has received institutional research support from Vifor Pharma, AstraZeneca, Ionis, Pfizer, Pharma Nord. N.G.B. received consulting fees from Vifor Pharma. P.v.d.M. received consulting fees from Vifor Pharma, Pharmacosmos and Novartis. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results. All other authors have no relationships to disclose that could be construed as a conflict of interest.
Figures
References
-
- Mamas M.A., Sperrin M., Watson M.C., Coutts A., Wilde K., Burton C., Kadam U.T., Kwok C.S., Clark A.B., Murchie P., et al. Do patients have worse outcomes in heart failure than in cancer? A primary care-based cohort study with 10-year follow-up in Scotland. Eur. J. Heart Fail. 2017;19:1095–1104. doi: 10.1002/ejhf.822. - DOI - PubMed
-
- Conrad N., Judge A., Tran J., Mohseni H., Hedgecott D., Crespillo A.P., Allison M., Hemingway H., Cleland J.G., McMurray J.J.V., et al. Temporal trends and patterns in heart failure incidence: A population-based study of 4 million individuals. Lancet. 2018;391:572–580. doi: 10.1016/S0140-6736(17)32520-5. - DOI - PMC - PubMed
-
- Braunstein J.B., Anderson G.F., Gerstenblith G., Weller W., Niefeld M., Herbert R., Wu A.W. Noncardiac comorbidity increases preventable hospitalizations and mortality among medicare beneficiaries with chronic heart failure. J. Am. Coll. Cardiol. 2003;42:1226–1233. doi: 10.1016/S0735-1097(03)00947-1. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
