

Gouty Arthropathy: Review of Clinical Manifestations and Treatment, with Emphasis on Imaging
- PMID: 35011907
- PMCID: PMC8745871
- DOI: 10.3390/jcm11010166
Gouty Arthropathy: Review of Clinical Manifestations and Treatment, with Emphasis on Imaging
Abstract
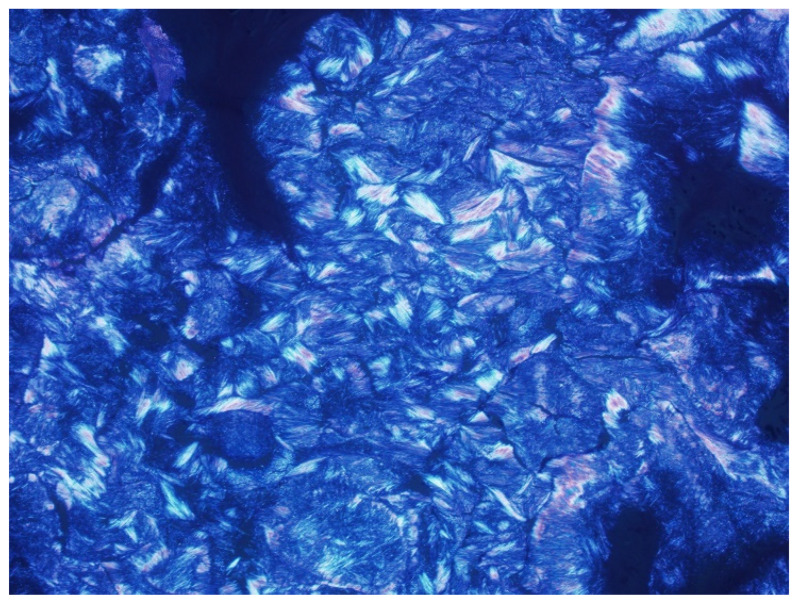
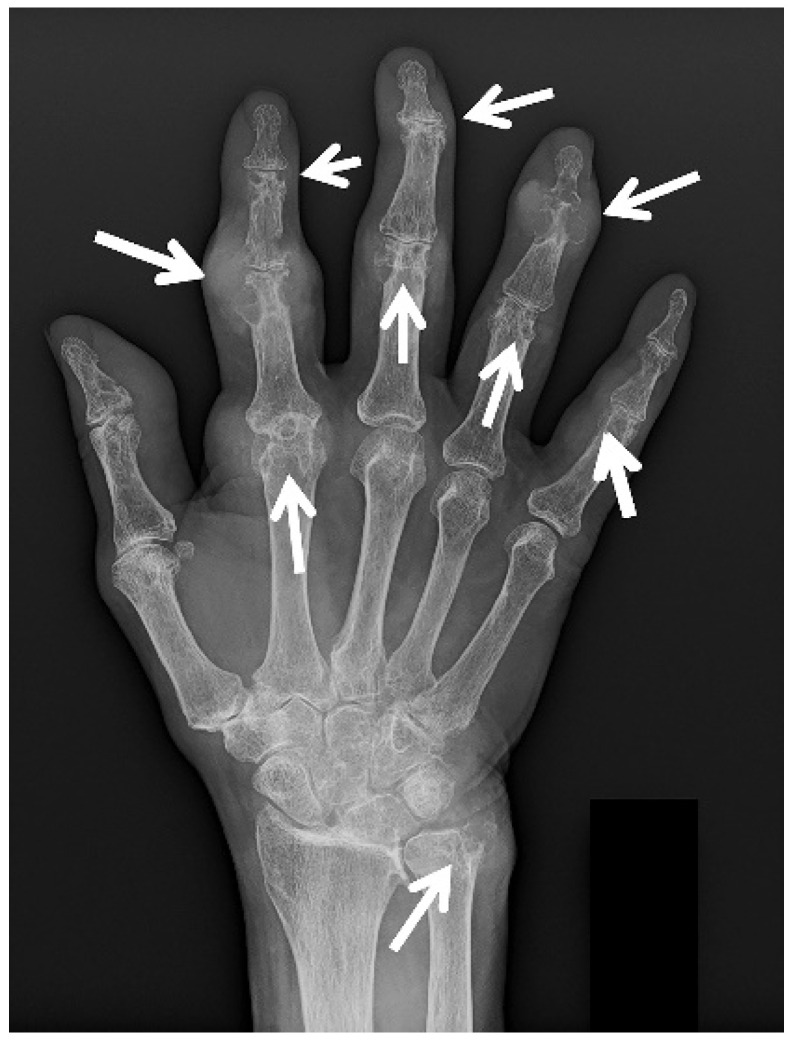
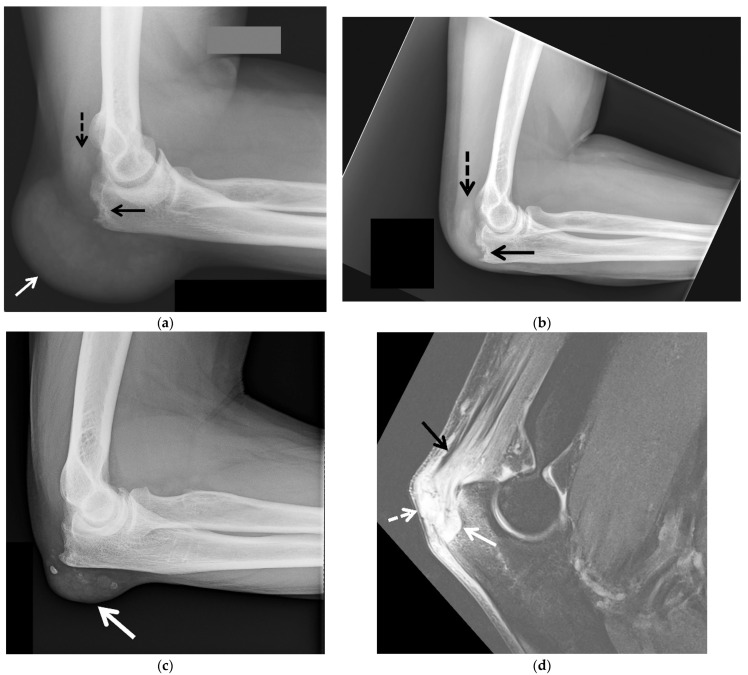
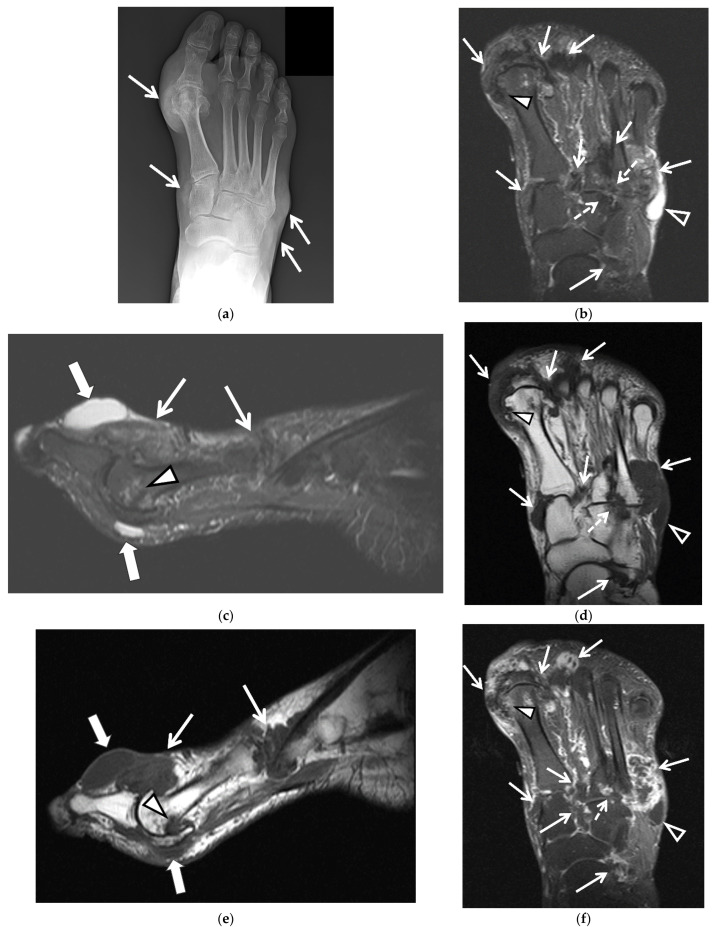
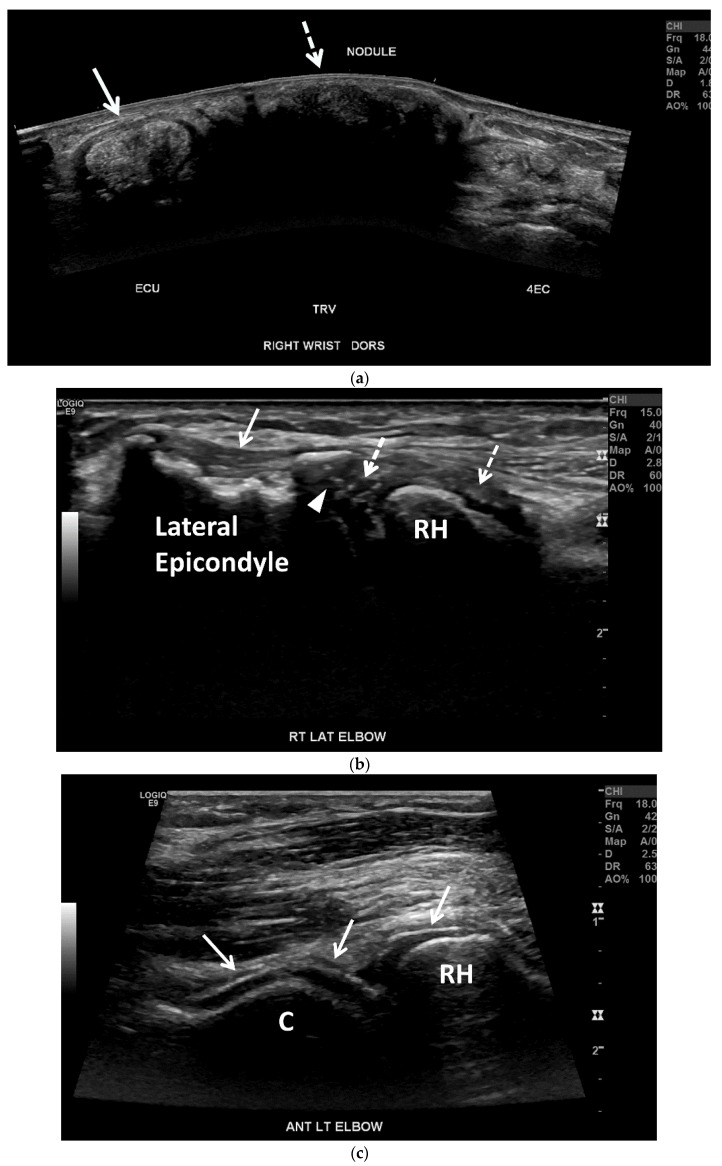
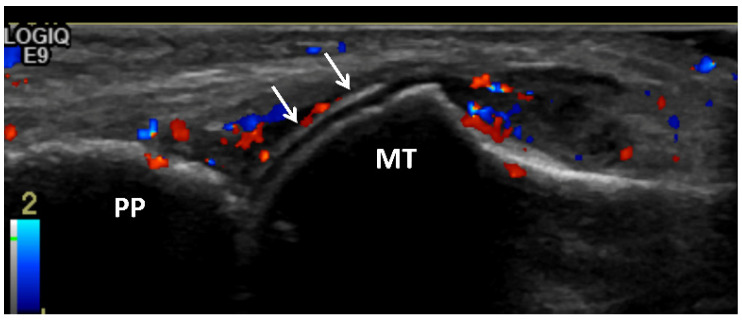
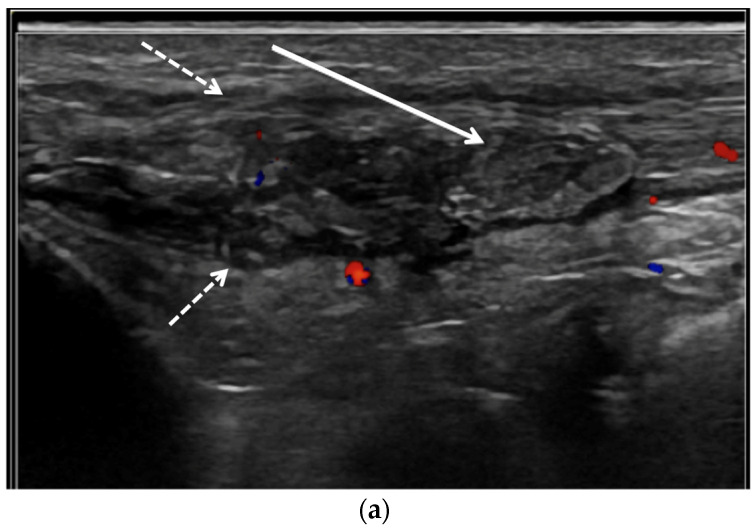
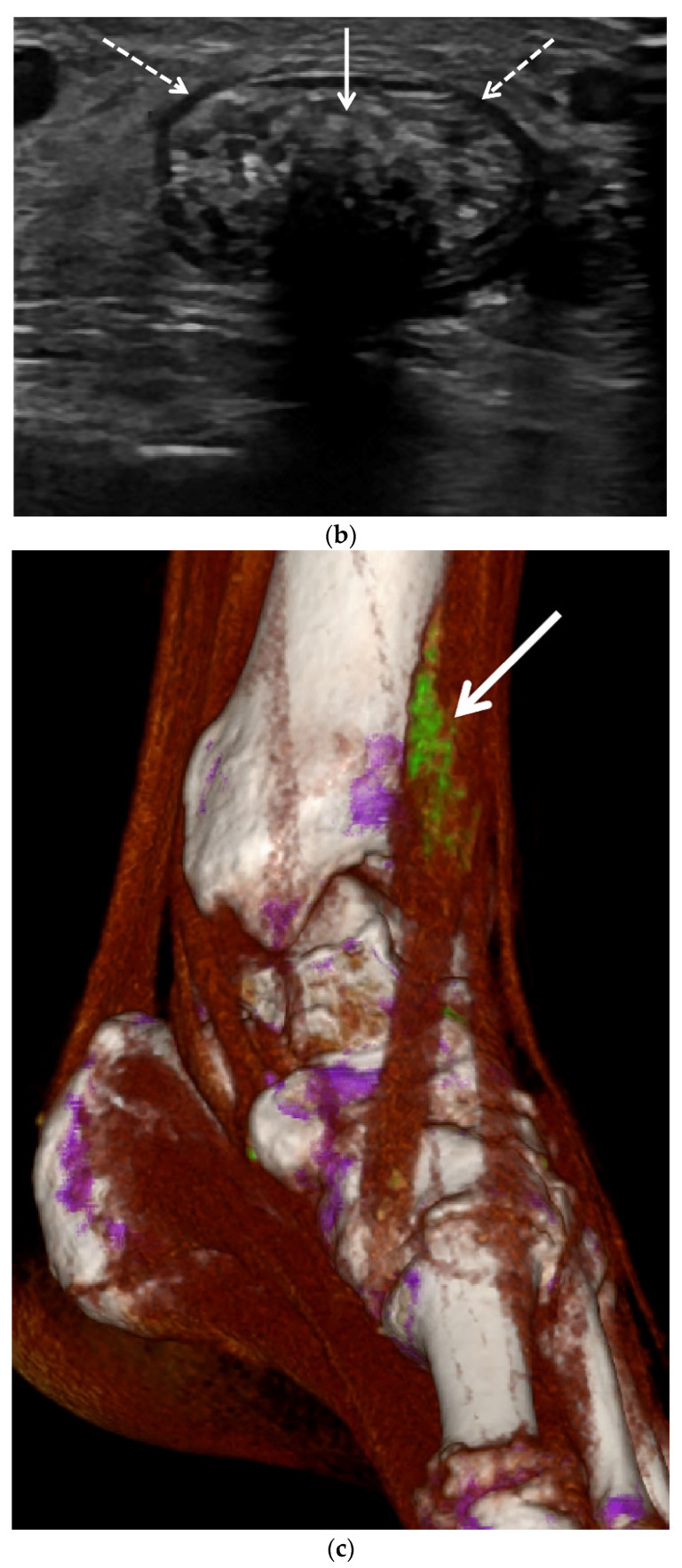
Gout, a crystalline arthropathy caused by the deposition of monosodium urate crystals in the articular and periarticular soft tissues, is a frequent cause of painful arthropathy. Imaging has an important role in the initial evaluation as well as the treatment and follow up of gouty arthropathy. The imaging findings of gouty arthropathy on radiography, ultrasonography, computed tomography, dual energy computed tomography, and magnetic resonance imaging are described to include findings of the early, acute and chronic phases of gout. These findings include early monosodium urate deposits, osseous erosions, and tophi, which may involve periarticular tissues, tendons, and bursae. Treatment of gout includes non-steroidal anti-inflammatories, colchicine, glucocorticoids, interleukin-1 inhibitors, xanthine oxidase inhibitors, uricosuric drugs, and recombinant uricase. Imaging is critical in monitoring response to therapy; clinical management can be modulated based on imaging findings. This review article describes the current standard of care in imaging and treatment of gouty arthropathy.
Keywords: CT; crystalline arthropathy; dual energy CT; gout; imaging; magnetic resonance imaging; monosodium urate crystals; radiography; sonography; treatment.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Neogi T., Jansen T.L., Dalbeth N., Fransen J., Schumacher H.R., Berendsen D., Brown M., Choi H., Edwards N.L., Janssens H.J., et al. 2015 Gout Classification Criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheumatol. 2015;67:2557–2568. doi: 10.1002/art.39254. - DOI - PMC - PubMed
-
- Taylor W.J., Fransen J., Jansen T.L., Dalbeth N., Schumacher H.R., Brown M., Louthrenoo W., Vazquez-Mellado J., Eliseev M., McCarthy G., et al. Study for Updated Gout Classification Criteria: Identification of Features to Classify Gout. Arthritis Care Res. (Hoboken) 2015;67:1304–1315. doi: 10.1002/acr.22585. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
