

Surgery and Catheter Ablation for Atrial Fibrillation: History, Current Practice, and Future Directions
- PMID: 35011953
- PMCID: PMC8745682
- DOI: 10.3390/jcm11010210
Surgery and Catheter Ablation for Atrial Fibrillation: History, Current Practice, and Future Directions
Abstract
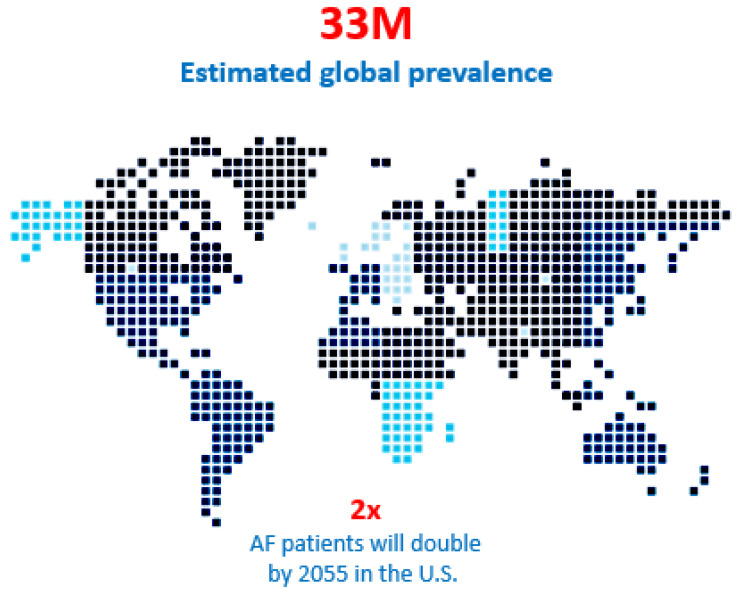
Atrial fibrillation (AF) is the most common of all cardiac arrhythmias, affecting roughly 1% of the general population in the Western world. The incidence of AF is predicted to double by 2050. Most patients with AF are treated with oral medications and only approximately 4% of AF patients are treated with interventional techniques, including catheter ablation and surgical ablation. The increasing prevalence and the morbidity/mortality associated with AF warrants a more aggressive approach to its treatment. It is the purpose of this invited editorial to describe the past, present, and anticipated future directions of the interventional therapy of AF, and to crystallize the problems that remain.
Keywords: atrial fibrillation; catheter ablation; electrophysiologic mapping; maze procedure.
Conflict of interest statement
McCarthy: Edwards Lifesciences: royalties and speaking fees; AtriCure and Medtronic: speaking fees. Cox: Consultant and Stockholder: AtriCure, Inc. and SentreHEART, Inc.; consultant, stockholder, and board of directors: Adagio Medical, Inc., PAVmed, Inc., Lucid Diagnostics, Inc. All other authors declare no conflict of interest.
Figures

References
-
- Chugh S.S., Havmoeller R., Narayanan K., Singh D., Rienstra M., Benjamin E.J., Gillum R.F., Kim Y.H., McAnulty J.H., Jr., Zheng Z.J., et al. Worldwide epidemiology of atrial fibrillation: A Global Burden of Disease 2010 Study. Circulation. 2014;129:837–847. doi: 10.1161/CIRCULATIONAHA.113.005119. - DOI - PMC - PubMed
-
- Steinberg B.A., Holmes D.N., Ezekowitz M.D., Fonarow G.C., Kowey P.R., Mahaffey K.W., Naccarelli G., Reiffel J., Chang P., Peterson E.D., et al. Rate versus rhythm control for management of atrial fibrillation in clinical practice: Results from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF) registry. Am. Heart J. 2013;165:622–629. doi: 10.1016/j.ahj.2012.12.019. - DOI - PMC - PubMed
-
- Calkins H., Reynolds M.R., Spector P., Sondhi M., Xu Y., Martin A., Williams C.J., Sledge I. Treatment of atrial fibrillation with antiarrhythmic drugs or radiofrequency ablation: Two systematic literature reviews and meta-analyses. Circ. Arrhythm. Electrophysiol. 2009;2:349–361. doi: 10.1161/CIRCEP.108.824789. - DOI - PubMed
-
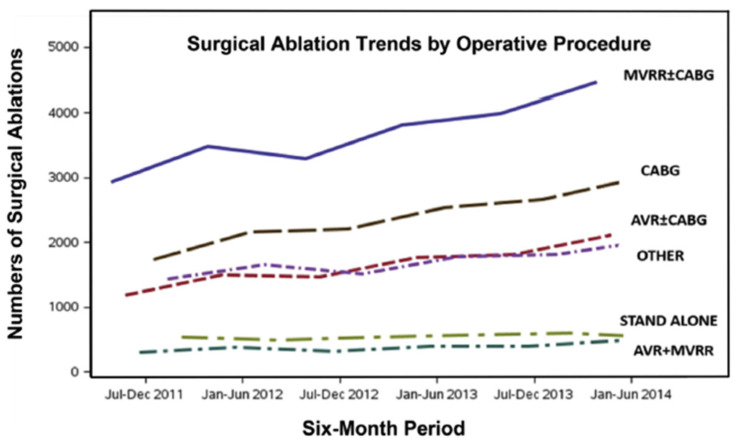
- Badhwar V., Rankin J.S., Ad N., Grau-Sepulveda M., Damiano R.J., Gillinov A.M., McCarthy P.M., Thourani V.H., Suri R.M., Jacobs J.P., et al. Surgical Ablation of Atrial Fibrillation in the United States: Trends and Propensity Matched Outcomes. Ann. Thorac. Surg. 2017;104:493–500. doi: 10.1016/j.athoracsur.2017.05.016. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
