

ONLINE-TICS: Internet-Delivered Behavioral Treatment for Patients with Chronic Tic Disorders
- PMID: 35011989
- PMCID: PMC8745756
- DOI: 10.3390/jcm11010250
ONLINE-TICS: Internet-Delivered Behavioral Treatment for Patients with Chronic Tic Disorders
Abstract
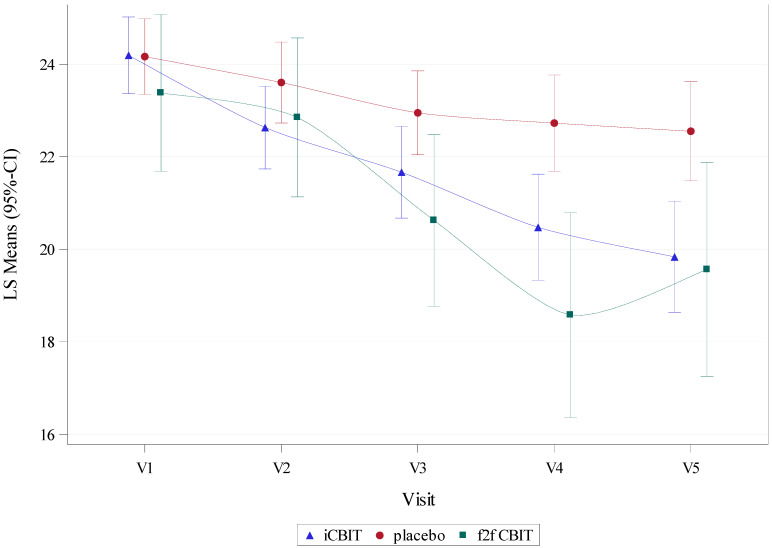
Comprehensive Behavioral Intervention for Tics (CBIT) is considered a first-line therapy for tics. However, availability of CBIT is extremely limited due to a lack of qualified therapists. This study is a multicenter (n = 5), randomized, controlled, observer-blind trial including 161 adult patients with chronic tic disorders (CTD) to provide data on efficacy and safety of an internet-delivered, completely therapist-independent CBIT intervention (iCBIT Minddistrict®) in the treatment of tics compared to placebo and face-to-face (f2f) CBIT. Using a linear mixed model with the change to baseline of Yale Global Tic Severity Scale-Total Tic Score (YGTSS-TTS) as a dependent variable, we found a clear trend towards significance for superiority of iCBIT (n = 67) over placebo (n = 70) (-1.28 (-2.58; 0.01); p = 0.053). In addition, the difference in tic reduction between iCBIT and placebo increased, resulting in a significant difference 3 (-2.25 (-3.75; -0.75), p = 0.003) and 6 months (-2.71 (-4.27; -1.16), p < 0.001) after the end of treatment. Key secondary analysis indicated non-inferiority of iCBIT in comparison to f2f CBIT (n = 24). No safety signals were detected. Although the primary endpoint was narrowly missed, it is strongly suggested that iCBIT is superior compared to placebo. Remarkably, treatment effects of iCBIT even increased over time.
Keywords: Comprehensive Behavioral Intervention for Tics (CBIT); Internet-Delivered Comprehensive Behavioral Intervention for Tics (iCBIT); Tourette syndrome; habit reversal training (HRT); tele-health; tics.
Conflict of interest statement
K.M.-V. has received financial or material research support from EU (FP7-HEALTH-2011 No. 278367, FP7-PEOPLE-2012-ITN No. 316978), DFG: GZ MU 1527/3-1 and GZ MU 1527/3-2, BMBF: 01KG1421, National Institute of Mental Health (NIMH), Tourette Gesellschaft Deutschland e.V., Else-Kröner-Fresenius-Stiftung, GW pharmaceuticals, Almirall Hermal GmbH, Abide Therapeutics, and Therapix Biosiences. She has received consultant’s honoraria from Abide Therapeutics, Boehringer Ingelheim International GmbH, Bionorica Ethics GmbH, CannaMedical Pharma GmbH, Canopy Grouth, Columbia Care, CTC Communications Corp., Demecan, Ethypharm GmbH, Eurox Deutschland GmbH, Global Praxis Group Limited, Lundbeck, MCI Germany, Neuraxpharm, Sanity Group, Stadapharm GmbH, Synendos Therapeutics AG, and Tilray. She is an advisory/scientific board member for Alexion, CannaMedical Pharma GmbH, Bionorica Ethics GmbH, CannaXan GmbH, Canopy Growth, Columbia Care, Ethypharm GmbH, IMC Germany, Leafly Deutschland GmbH, Neuraxpharm, Sanity Group, Stadapharm GmbH, Synendos Therapeutics AG, Syqe Medical Ltd., Therapix Biosciences Ltd., Tilray, von Mende Marketing GmbH, Wayland Group, and Zambon. She has received speaker’s fees from Aphria Deutschland GmbH, Almirall, Camurus, Cogitando GmbH, Emalex, Eurox Deutschland GmbH, Ever pharma GmbH, Meinhardt Congress GmbH, PR Berater, Spectrum Therapeutics GmbH, Takeda GmbH, Tilray, and Wayland Group. She has received royalties from Deutsches Ärzteblatt, Der Neurologie und Psychiater, Elsevier, Medizinisch Wissenschaftliche Verlagsgesellschaft Berlin, and Kohlhammer. She served as a guest editor for Frontiers in Neurology on the research topic “The neurobiology and genetics of Gilles de la Tourette syndrome: new avenues through large-scale collaborative projects”, is an associate editor for “Cannabis and Cannabinoid Research” and an editorial board member of “Medical Cannabis and Cannabinoids” and “MDPI-Reports”, and is a scientific board member for “Zeitschrift für Allgemeinmedizin”. R.M. received speakers’ honoraria from Otsuka Pharmaceuticals and Lundbeck. He received funding as PI for clinical trials conducted by Böhringer-Ingelheim, Otsuka Pharmaceuticals, EMALEX Biosciences, and TEVA GmbH. V.R. has received payment for consulting and writing activities from Lilly, Novartis, and Shire Pharmaceuticals, lecture honoraria from Lilly, Novartis, Shire Pharmaceuticals, and Medice Pharma, and support for research from Shire Pharmaceuticals and Novartis. He has carried out clinical trials in cooperation with the Novartis, Shire, Servier and Otsuka companies. I.R. has received funding from Janssen-Cilag GmbH as PI for clinical trials. All other authors declare no conflict of interest. The funder (BMBF) had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
References
-
- American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Association; Arlington, VA, USA: 2013.
Grants and funding
LinkOut - more resources
Full Text Sources
