

Evaluation of Brace Treatment Using the Soft Brace Spinaposture: A Four-Years Follow-Up
- PMID: 35012005
- PMCID: PMC8745903
- DOI: 10.3390/jcm11010264
Evaluation of Brace Treatment Using the Soft Brace Spinaposture: A Four-Years Follow-Up
Abstract
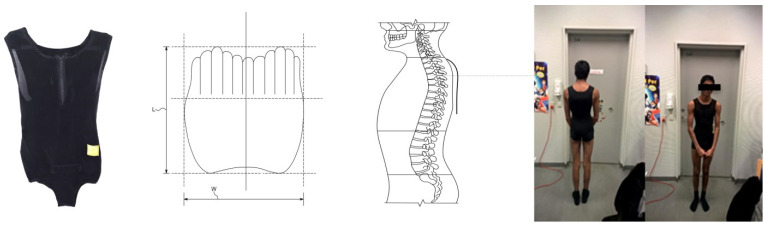
The braces of today are constructed to correct the frontal plane deformity of idiopathic adolescent scoliosis (AIS). The Spinaposture brace© (Spinaposture Aps, Copenhagen, Denmark) is a soft-fabric brace for AIS and is designed to enhance rotational axial stability by inducing a sagittal plane kyphotic correction. This prospective observational study evaluated the brace in fifteen patients with AIS. The initial average CA was 16.8° (SD: 2.8). They were followed prospectively every 3 to 6 months during their brace usage until skeletal maturity of 25 months and at long-term follow-up of 44 months. In- and out-of-brace radiographs were performed in six subjects at inclusion. This resulted in an immediate in-brace correction of 25.3 percent in CA (14.3°→10.8°) and induced a kyphotic effect of 14.9 percent (40.8°→47.9°). The average in-brace improvement at first follow-up was 4.5° in CA, and the CA at skeletal maturity was 11° (SD: 7.4°) and long-term 12.0° (SD: 6.8°). In conclusion, the Spinaposture brace© had an immediate in-brace deformity correction and a thoracic kyphotic effect. At skeletal maturity, the deformities improved more than expected when compared to that of the natural history/observation and similar to that of other soft braces. No long-term deformity progression was seen. To substantiate these findings, stronger designed studies with additional subjects are needed.
Keywords: bracing; follow-up study; idiopathic scoliosis; pathobiomechanics; spinal deformities.
Conflict of interest statement
The first author is part owner of the company with the patent for the Spinaposture brace. This company had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures





Similar articles
-
Preliminary evaluation of a computer-assisted tool for the design and adjustment of braces in idiopathic scoliosis: a prospective and randomized study.Spine (Phila Pa 1976). 2007 Apr 15;32(8):835-43. doi: 10.1097/01.brs.0000259811.58372.87. Spine (Phila Pa 1976). 2007. PMID: 17426626 Clinical Trial.
-
Adolescent idiopathic scoliosis, bracing, and the Hueter-Volkmann principle.Spine J. 2003 May-Jun;3(3):180-5. doi: 10.1016/s1529-9430(02)00557-0. Spine J. 2003. PMID: 14589197
-
Bracing for juvenile idiopathic scoliosis: retrospective review from bracing to skeletal maturity.Spine Deform. 2022 Nov;10(6):1349-1358. doi: 10.1007/s43390-022-00544-2. Epub 2022 Jul 19. Spine Deform. 2022. PMID: 35852786 Free PMC article.
-
Pediatric cervical kyphosis in the MRI era (1984-2008) with long-term follow up: literature review.Childs Nerv Syst. 2022 Feb;38(2):361-377. doi: 10.1007/s00381-021-05409-z. Epub 2021 Nov 22. Childs Nerv Syst. 2022. PMID: 34806157 Review.
-
Standardization of criteria for adolescent idiopathic scoliosis brace studies: SRS Committee on Bracing and Nonoperative Management.Spine (Phila Pa 1976). 2005 Sep 15;30(18):2068-75; discussion 2076-7. doi: 10.1097/01.brs.0000178819.90239.d0. Spine (Phila Pa 1976). 2005. PMID: 16166897 Review.
Cited by
-
Early outcomes in hybrid fixation for idiopathic scoliosis: posterior fusion combined with anterior vertebral body tethering. Patient series.J Neurosurg Case Lessons. 2023 Oct 9;6(15):CASE23331. doi: 10.3171/CASE23331. Print 2023 Oct 9. J Neurosurg Case Lessons. 2023. PMID: 37910004 Free PMC article.
References
-
- Nachemson A.L., Peterson L.E. Effectiveness of treatment with a brace in girls who have adolescent idiopathic scoliosis. A prospective, controlled study based on data from the Brace Study of the Scoliosis Research Society. J. Bone Jt. Surg. Am. 1995;77:815–822. doi: 10.2106/00004623-199506000-00001. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
