

Association between CHADS2, CHA2DS2-VASc, ATRIA, and Essen Stroke Risk Scores and Unsuccessful Recanalization after Endovascular Thrombectomy in Acute Ischemic Stroke Patients
- PMID: 35012015
- PMCID: PMC8746082
- DOI: 10.3390/jcm11010274
Association between CHADS2, CHA2DS2-VASc, ATRIA, and Essen Stroke Risk Scores and Unsuccessful Recanalization after Endovascular Thrombectomy in Acute Ischemic Stroke Patients
Abstract
Background: The CHADS2, CHA2DS2-VASc, ATRIA, and Essen scores have been developed for predicting vascular outcomes in stroke patients. We investigated the association between these stroke risk scores and unsuccessful recanalization after endovascular thrombectomy (EVT).
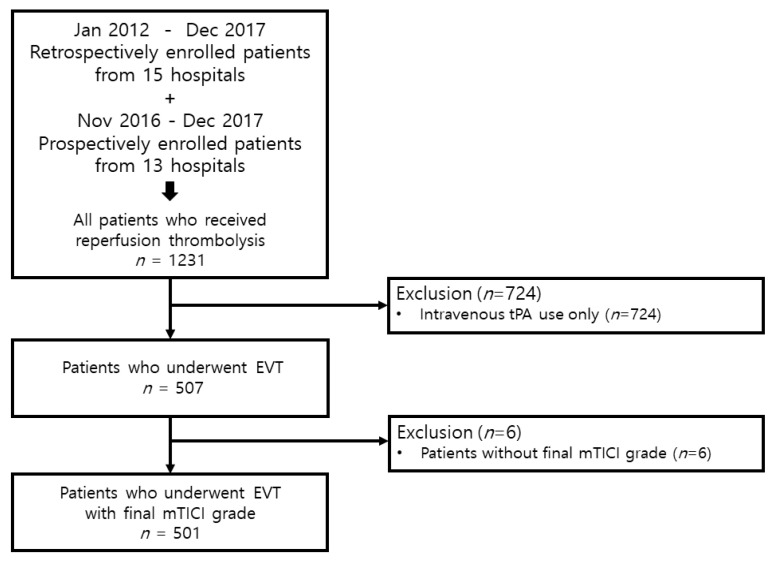
Methods: From the nationwide multicenter registry (Selection Criteria in Endovascular Thrombectomy and Thrombolytic therapy (SECRET)) (Clinicaltrials.gov NCT02964052), we consecutively included 501 patients who underwent EVT. We identified pre-admission stroke risk scores in each included patient.
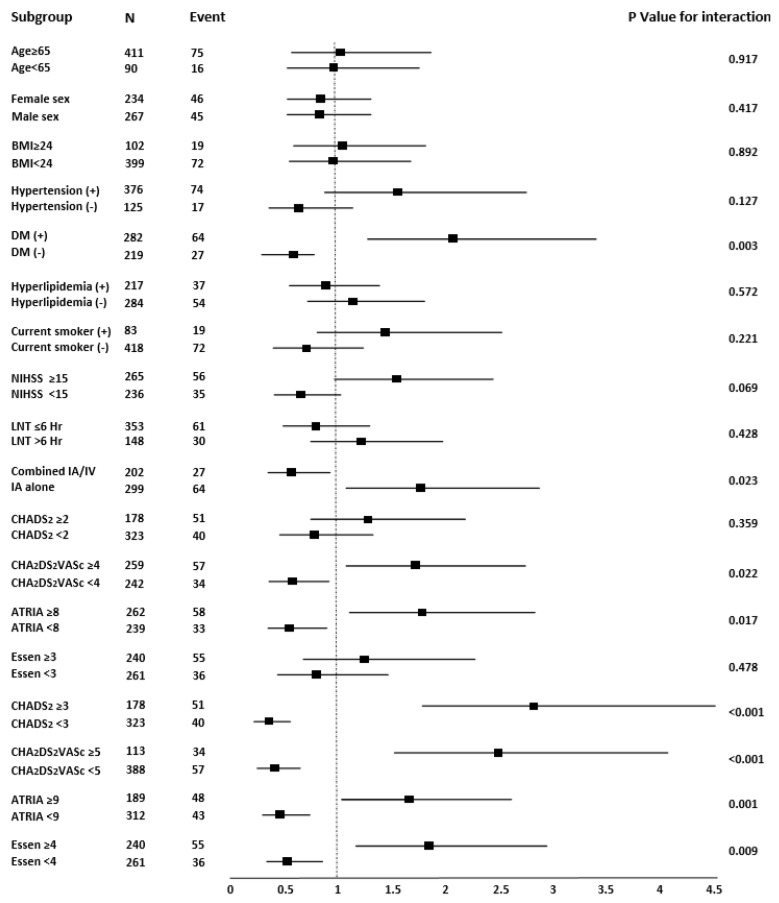
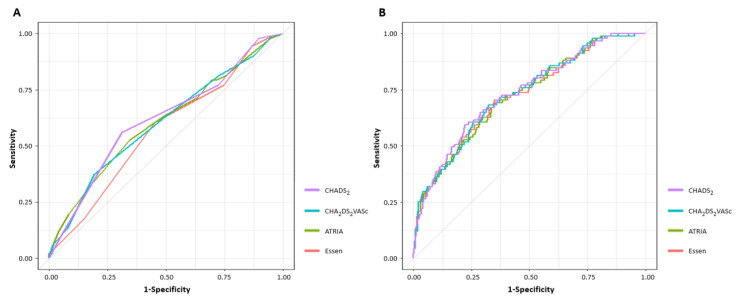
Results: Among 501 patients who underwent EVT, 410 (81.8%) patients achieved successful recanalization (mTICI ≥ 2b). Adjusting for body mass index and p < 0.1 in univariable analysis revealed the association between all stroke risk scores and unsuccessful recanalization (CHADS2 score: odds ratio (OR) 1.551, 95% confidence interval (CI) 1.198-2.009, p = 0.001; CHA2DS2VASc score: OR 1.269, 95% CI 1.080-1.492, p = 0.004; ATRIA score: OR 1.089, 95% CI 1.011-1.174, p = 0.024; and Essen score: OR 1.469, 95% CI 1.167-1.849, p = 0.001). The CHADS2 score had the highest AUC value and differed significantly only from the Essen score (AUC of CHADS2 score; 0.618, 95% CI 0.554-0.681).
Conclusion: All stroke risk scores were associated with unsuccessful recanalization after EVT. Our study suggests that these stroke risk scores could be used to predict recanalization in stroke patients undergoing EVT.
Keywords: ischemic stroke; recanalization; stroke risk score; thrombectomy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Association of CHA2DS2-VASc score with successful recanalization in acute ischemic stroke patients undergoing endovascular thrombectomy.Postepy Kardiol Interwencyjnej. 2022 Sep;18(3):269-275. doi: 10.5114/aic.2022.122027. Epub 2022 Dec 17. Postepy Kardiol Interwencyjnej. 2022. PMID: 36751289 Free PMC article.
-
Association between CHADS2, CHA2DS2-VASc, ATRIA, and Essen Stroke Risk Scores and Functional Outcomes in Acute Ischemic Stroke Patients Who Received Endovascular Thrombectomy.J Clin Med. 2022 Sep 23;11(19):5599. doi: 10.3390/jcm11195599. J Clin Med. 2022. PMID: 36233464 Free PMC article.
-
CHADS2, CHA2DS2-VASc, ATRIA, and Essen stroke risk scores in stroke with atrial fibrillation: A nationwide multicenter registry study.Medicine (Baltimore). 2021 Jan 22;100(3):e24000. doi: 10.1097/MD.0000000000024000. Medicine (Baltimore). 2021. PMID: 33545993 Free PMC article.
-
Pre-stroke CHADS2 and CHA2DS2-VASc scores are useful in stratifying three-month outcomes in patients with and without atrial fibrillation.Cerebrovasc Dis. 2013;36(4):273-80. doi: 10.1159/000353670. Epub 2013 Oct 16. Cerebrovasc Dis. 2013. PMID: 24135809
-
Meta-analysis of CHADS2 versus CHA2DS2-VASc for predicting stroke and thromboembolism in atrial fibrillation patients independent of anticoagulation.Tex Heart Inst J. 2015 Feb 1;42(1):6-15. doi: 10.14503/THIJ-14-4353. eCollection 2015 Feb. Tex Heart Inst J. 2015. PMID: 25873792 Free PMC article. Review.
Cited by
-
Outcomes and risk factors for infection after endovascular treatment in patients with acute ischemic stroke.CNS Neurosci Ther. 2024 May;30(5):e14753. doi: 10.1111/cns.14753. CNS Neurosci Ther. 2024. PMID: 38727582 Free PMC article.
-
Association of CHA2DS2-VASc score with successful recanalization in acute ischemic stroke patients undergoing endovascular thrombectomy.Postepy Kardiol Interwencyjnej. 2022 Sep;18(3):269-275. doi: 10.5114/aic.2022.122027. Epub 2022 Dec 17. Postepy Kardiol Interwencyjnej. 2022. PMID: 36751289 Free PMC article.
-
Advance of Thrombolysis and Thrombectomy in Acute Ischemic Stroke.J Clin Med. 2023 Jan 16;12(2):720. doi: 10.3390/jcm12020720. J Clin Med. 2023. PMID: 36675648 Free PMC article.
-
Association between CHADS2, CHA2DS2-VASc, ATRIA, and Essen Stroke Risk Scores and Functional Outcomes in Acute Ischemic Stroke Patients Who Received Endovascular Thrombectomy.J Clin Med. 2022 Sep 23;11(19):5599. doi: 10.3390/jcm11195599. J Clin Med. 2022. PMID: 36233464 Free PMC article.
References
-
- Ko S.-B., Park H.-K., Kim B.M., Heo J.H., Rha J.-H., Kwon S.U., Kim J.S., Lee B.-C., Suh S.H., Jung C., et al. 2019 Update of the Korean Clinical Practice Guidelines of Stroke for Endovascular Recanalization Therapy in Patients with Acute Ischemic Stroke. J. Stroke. 2019;21:231–240. doi: 10.5853/jos.2019.00024. - DOI - PMC - PubMed
-
- Albers G.W., Marks M.P., Kemp S., Christensen S., Tsai J.P., Ortega-Gutierrez S., McTaggart R.A., Torbey M.T., Kim-Tenser M., Leslie-Mazwi T., et al. Thrombectomy for Stroke at 6 to 16 Hours with Selection by Perfusion Imaging. N. Engl. J. Med. 2018;378:708–718. doi: 10.1056/NEJMoa1713973. - DOI - PMC - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
