

Artificial intelligence framework identifies candidate targets for drug repurposing in Alzheimer's disease
- PMID: 35012639
- PMCID: PMC8751379
- DOI: 10.1186/s13195-021-00951-z
Artificial intelligence framework identifies candidate targets for drug repurposing in Alzheimer's disease
Abstract
Background: Genome-wide association studies (GWAS) have identified numerous susceptibility loci for Alzheimer's disease (AD). However, utilizing GWAS and multi-omics data to identify high-confidence AD risk genes (ARGs) and druggable targets that can guide development of new therapeutics for patients suffering from AD has heretofore not been successful.
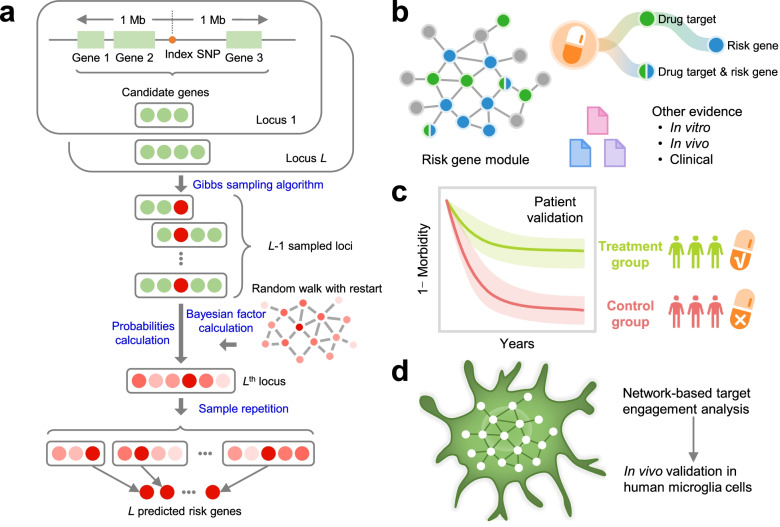
Methods: To address this critical problem in the field, we have developed a network-based artificial intelligence framework that is capable of integrating multi-omics data along with human protein-protein interactome networks to accurately infer accurate drug targets impacted by GWAS-identified variants to identify new therapeutics. When applied to AD, this approach integrates GWAS findings, multi-omics data from brain samples of AD patients and AD transgenic animal models, drug-target networks, and the human protein-protein interactome, along with large-scale patient database validation and in vitro mechanistic observations in human microglia cells.
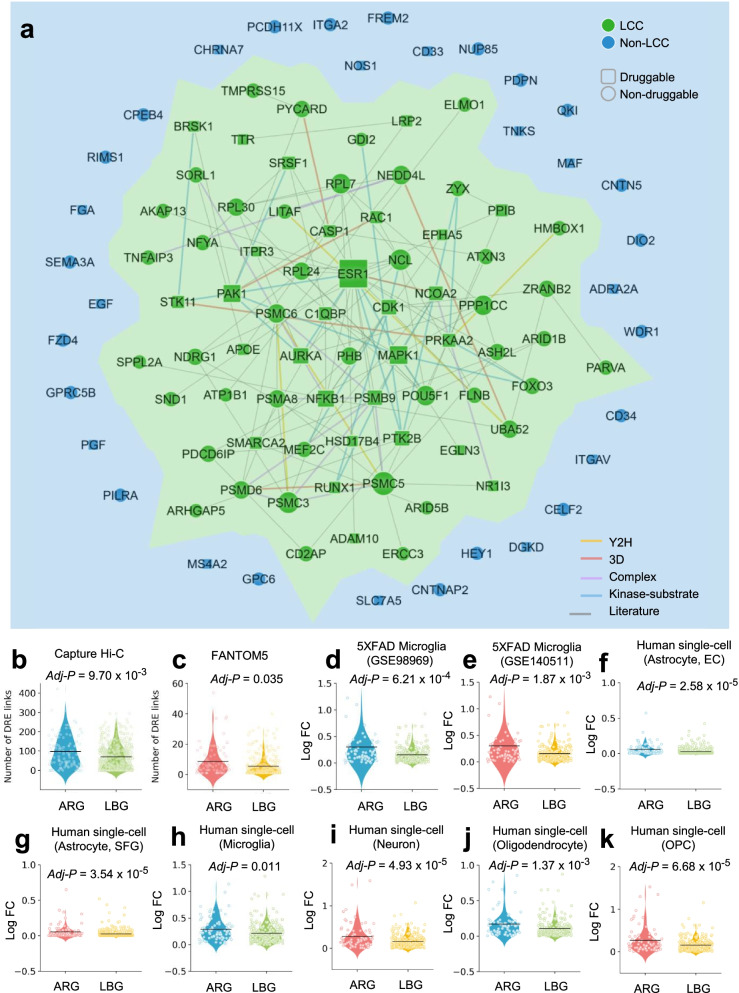
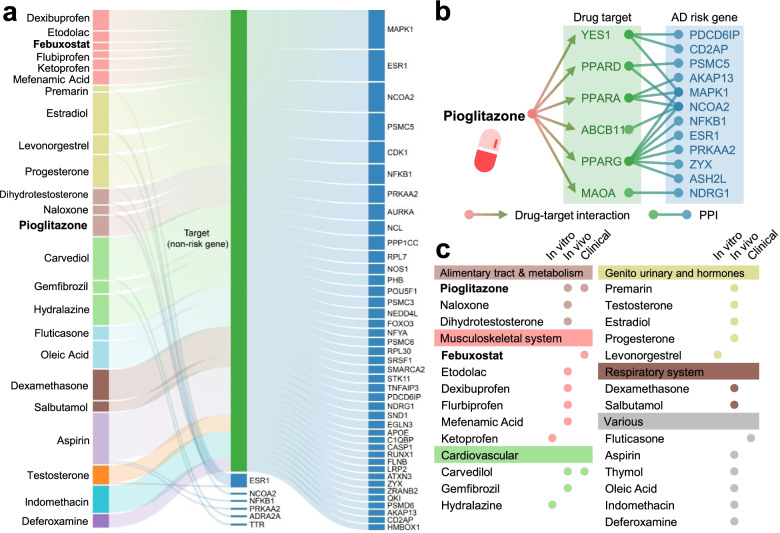
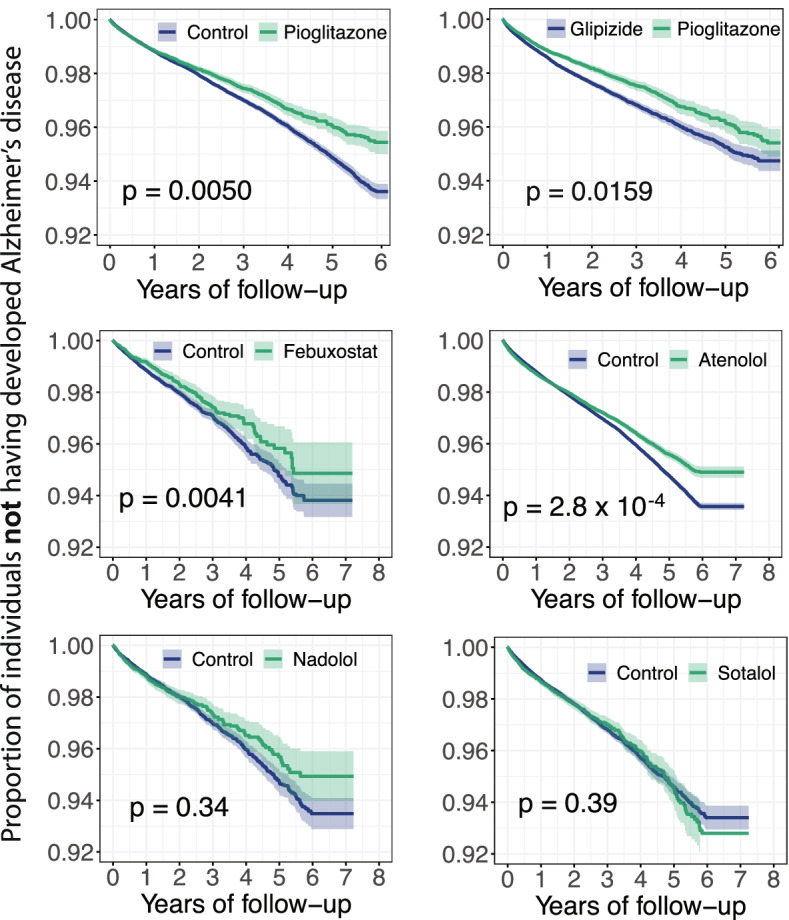
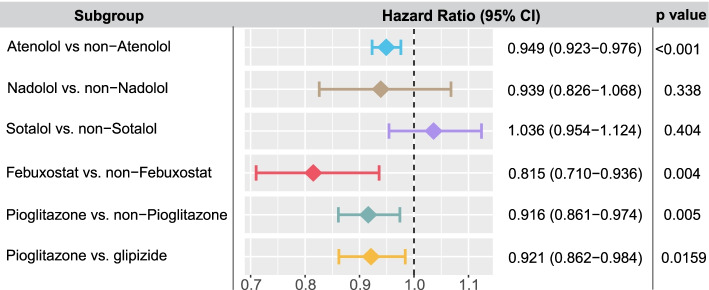
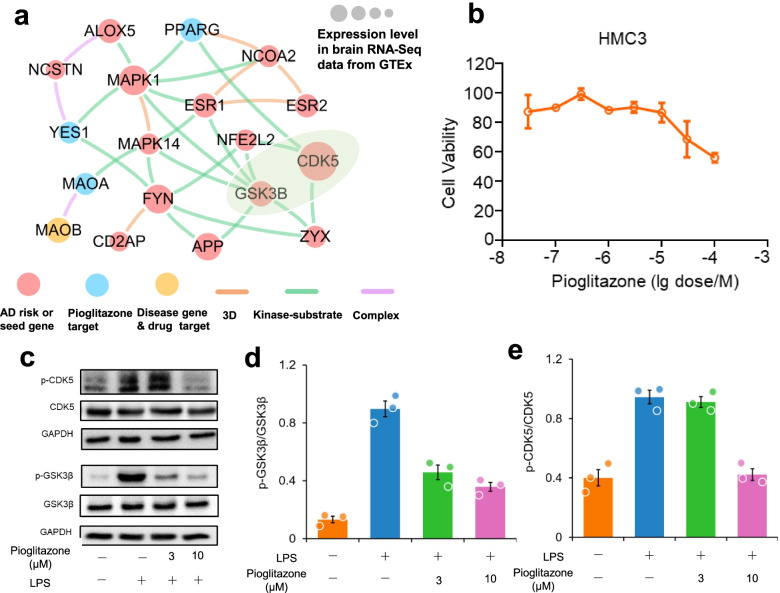
Results: Through this approach, we identified 103 ARGs validated by various levels of pathobiological evidence in AD. Via network-based prediction and population-based validation, we then showed that three drugs (pioglitazone, febuxostat, and atenolol) are significantly associated with decreased risk of AD compared with matched control populations. Pioglitazone usage is significantly associated with decreased risk of AD (hazard ratio (HR) = 0.916, 95% confidence interval [CI] 0.861-0.974, P = 0.005) in a retrospective case-control validation. Pioglitazone is a peroxisome proliferator-activated receptor (PPAR) agonist used to treat type 2 diabetes, and propensity score matching cohort studies confirmed its association with reduced risk of AD in comparison to glipizide (HR = 0.921, 95% CI 0.862-0.984, P = 0.0159), an insulin secretagogue that is also used to treat type 2 diabetes. In vitro experiments showed that pioglitazone downregulated glycogen synthase kinase 3 beta (GSK3β) and cyclin-dependent kinase (CDK5) in human microglia cells, supporting a possible mechanism-of-action for its beneficial effect in AD.
Conclusions: In summary, we present an integrated, network-based artificial intelligence methodology to rapidly translate GWAS findings and multi-omics data to genotype-informed therapeutic discovery in AD.
Keywords: Alzheimer’s disease; Drug repurposing; Genome-wide association studies (GWAS); Multi-omics; Network medicine; Pioglitazone.
© 2022. The Author(s).
Conflict of interest statement
Dr. Cummings has provided consultation to Acadia, Actinogen, Alkahest, Alzheon, Annovis, Avanir, Axsome, Biogen, BioXcel, Cassava, Cerecin, Cerevel, Cortexyme, Cytox, EIP Pharma, Eisai, Foresight, GemVax, Genentech, Green Valley, Grifols, Karuna, Merck, Novo Nordisk, Otsuka, Resverlogix, Roche, Samumed, Samus, Signant Health, Suven, Third Rock, and United Neuroscience pharmaceutical and assessment companies. Dr. Cummings has stock options in ADAMAS, AnnovisBio, MedAvante, and BiOasis. Dr. Leverenz has received consulting fees from Vaxxinity, grant support from GE Healthcare and serves on a Data Safety Monitoring Board for Eisai. The other authors declare that they have no competing interests.
Figures

References
-
- Masters CL, Bateman R, Blennow K, Rowe CC, Sperling RA, Cummings JL. Alzheimer's disease. Nat Rev Dis Primers. 2015;1:15056. 10.1038/nrdp.2015.56 pmid: 27188934. - PubMed
-
- Nichols E, Szoeke CEI, Vollset SE, Abbasi N, Abd-Allah F, Abdela J. Global, regional, and national burden of Alzheimer's disease and other dementias, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(1):88-106. 10.1016/s1474-4422(18)30403-4 pmid: 30497964. - PMC - PubMed
-
- Cuyvers E, Sleegers K. Genetic variations underlying Alzheimer's disease: evidence from genome-wide association studies and beyond. Lancet Neurol. 2016;15(8):857-68. 10.1016/s1474-4422(16)00127-7 pmid: 27302364. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 AG069900/AG/NIA NIH HHS/United States
- R35 AG071476/AG/NIA NIH HHS/United States
- P30AG072959/AG/NIA NIH HHS/United States
- U01 AG073323/AG/NIA NIH HHS/United States
- R01 AG066707/AG/NIA NIH HHS/United States
- P30 AG072959/AG/NIA NIH HHS/United States
- R35AG71476/AG/NIA NIH HHS/United States
- R56AG063870/AG/NIA NIH HHS/United States
- R56 AG063870/AG/NIA NIH HHS/United States
- P20 AG068053/AG/NIA NIH HHS/United States
- R56 AG074001/AG/NIA NIH HHS/United States
- R01AG069900/AG/NIA NIH HHS/United States
- P20 GM109025/GM/NIGMS NIH HHS/United States
- R01AG066707/AG/NIA NIH HHS/United States
