

Preclinical and randomized phase I studies of plitidepsin in adults hospitalized with COVID-19
- PMID: 35012962
- PMCID: PMC8761492
- DOI: 10.26508/lsa.202101200
Preclinical and randomized phase I studies of plitidepsin in adults hospitalized with COVID-19
Abstract
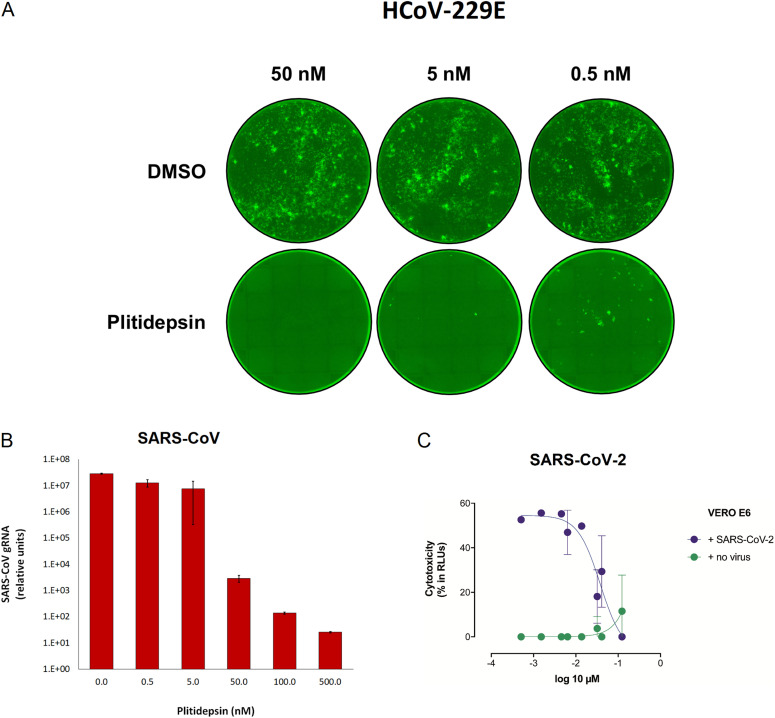
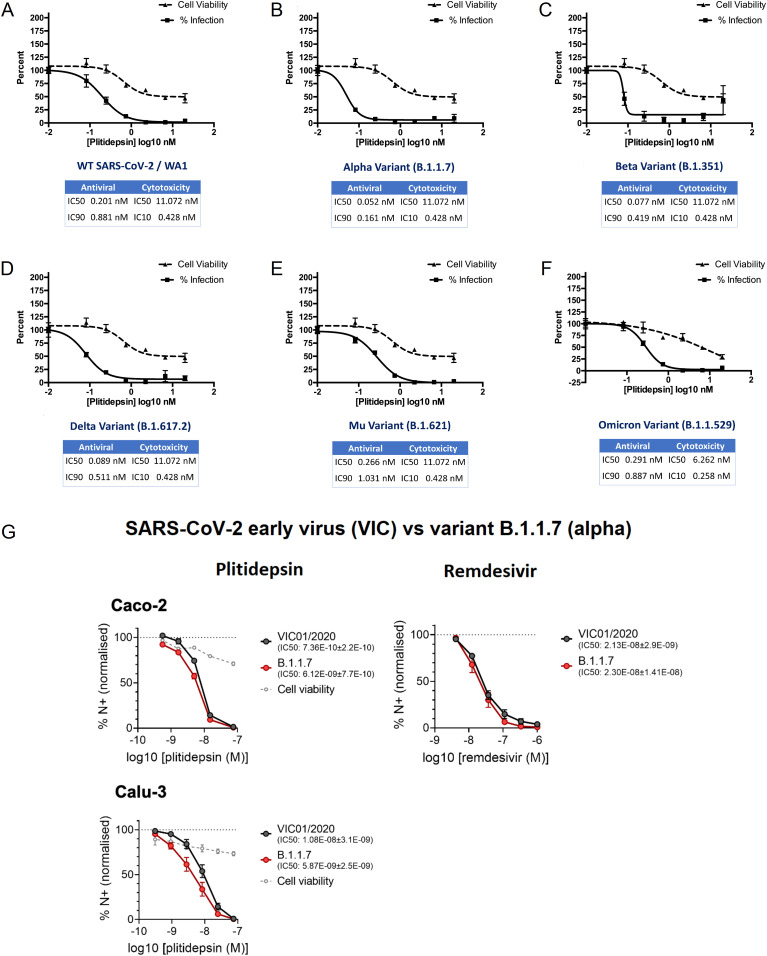
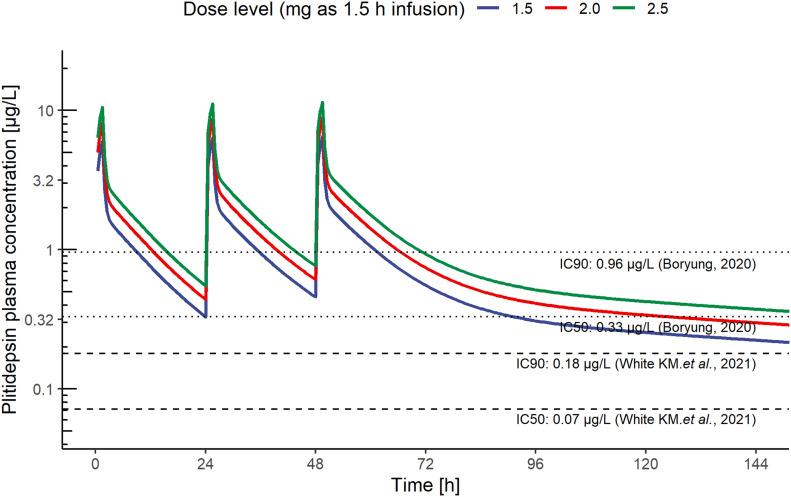
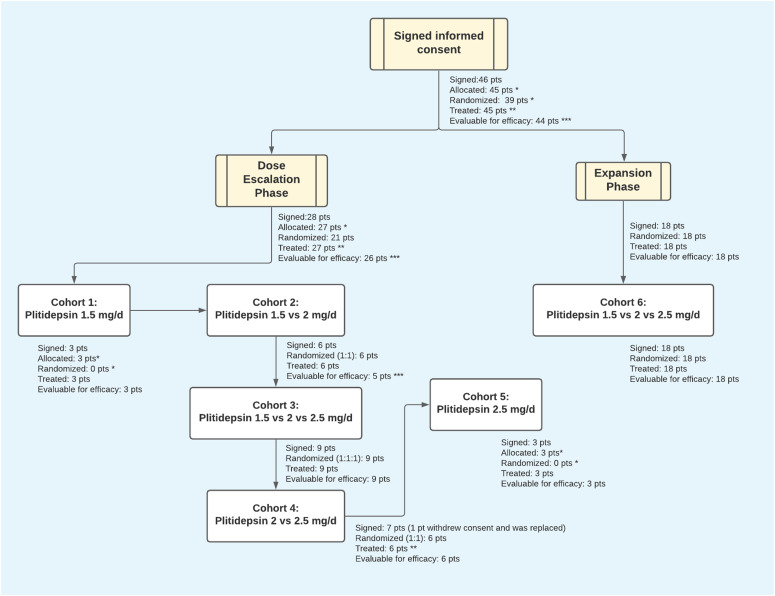
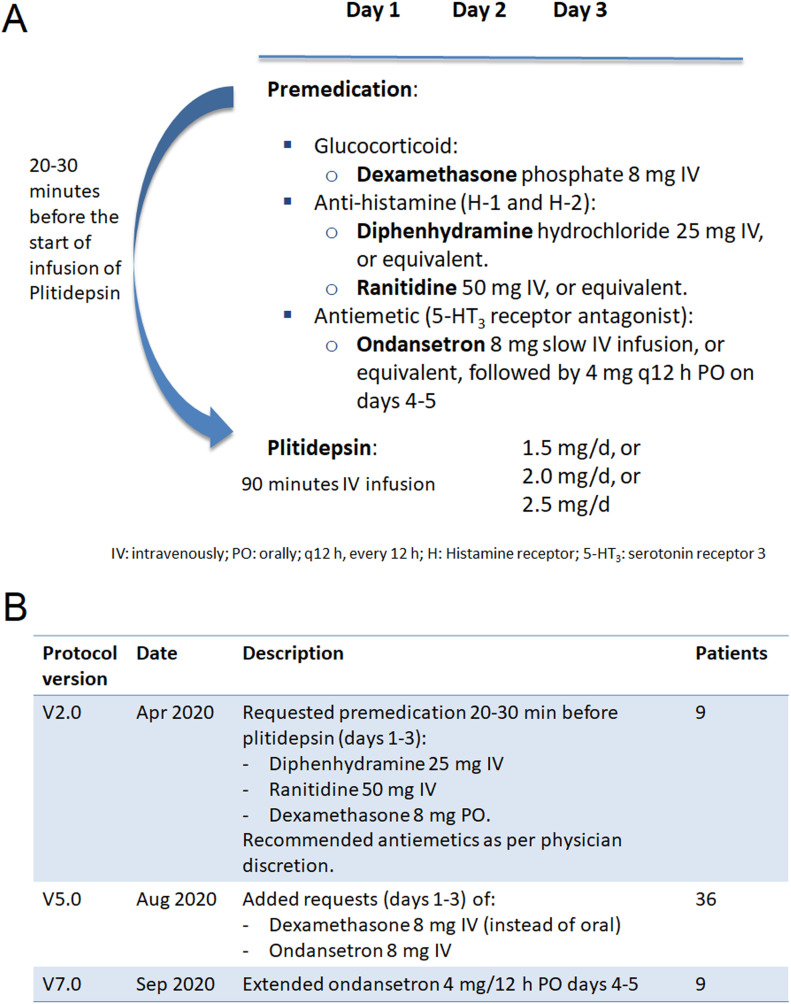
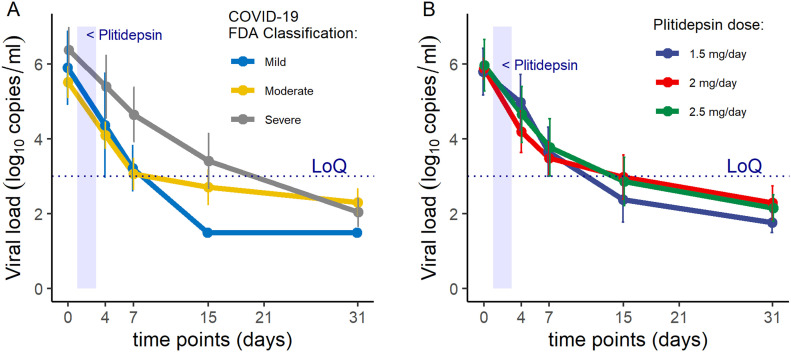
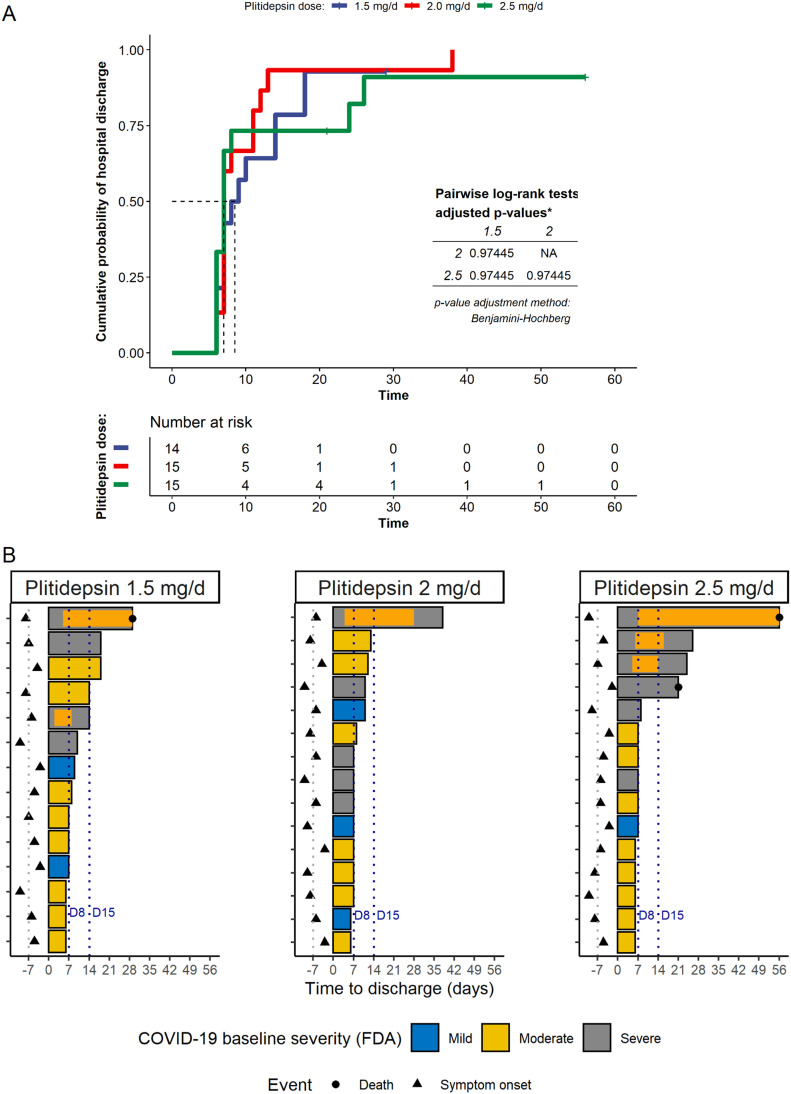
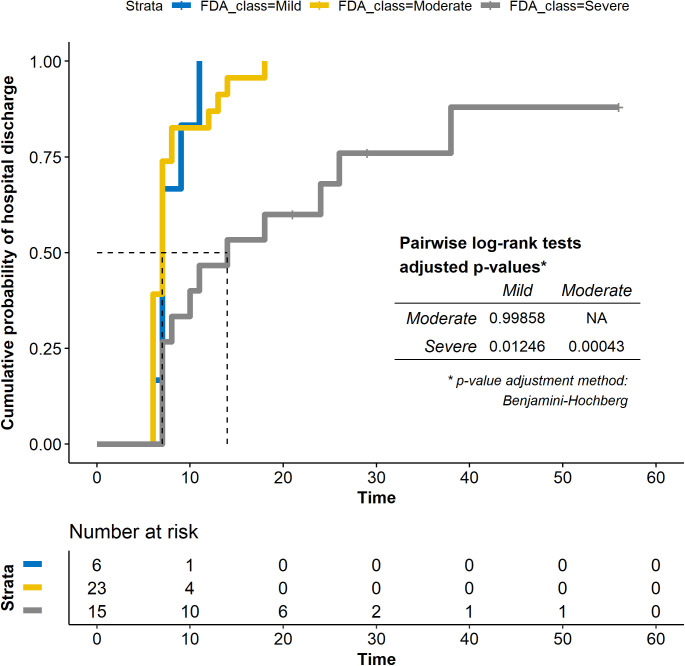
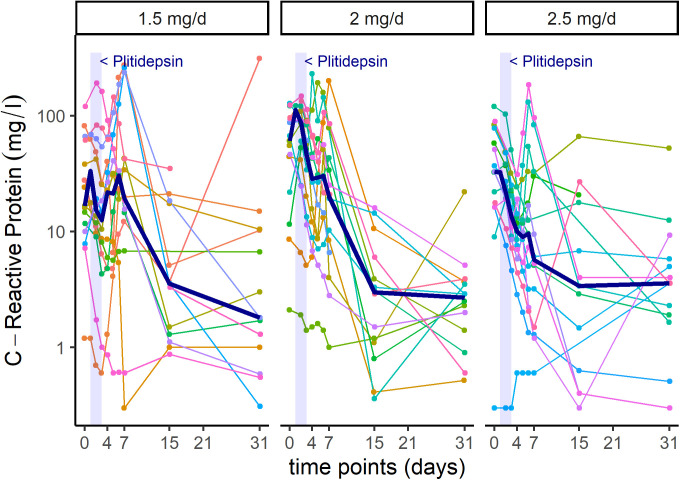
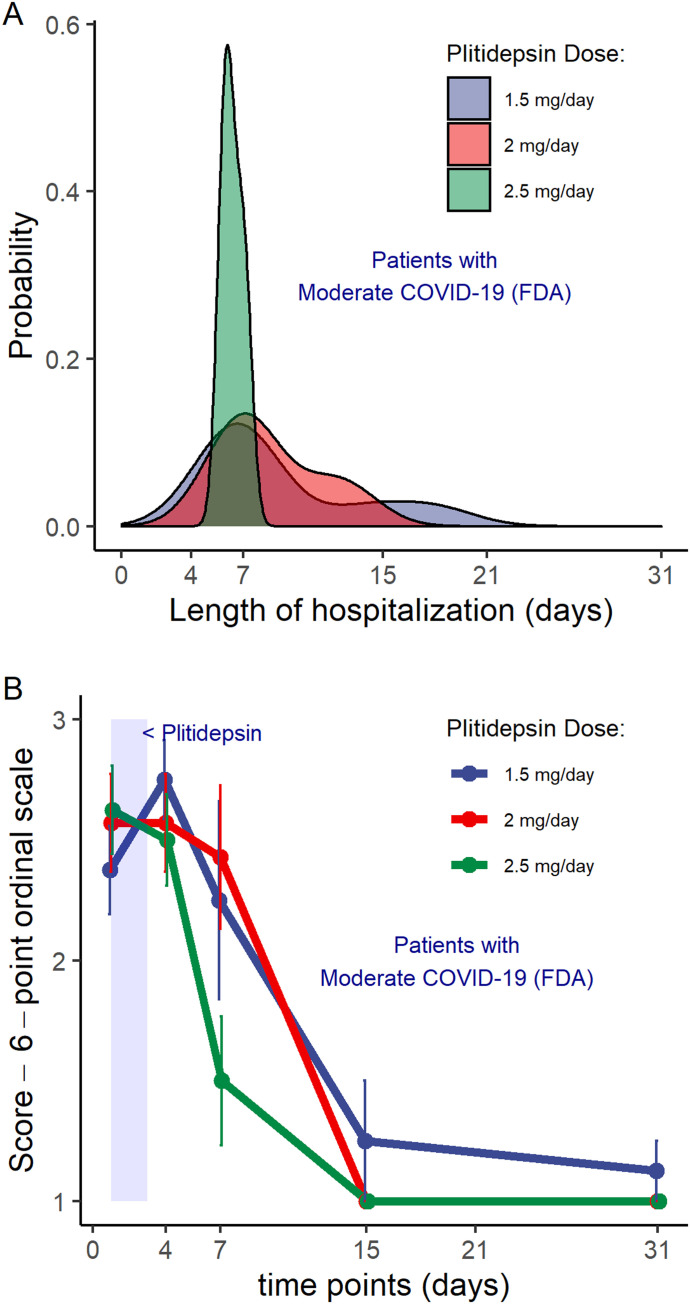
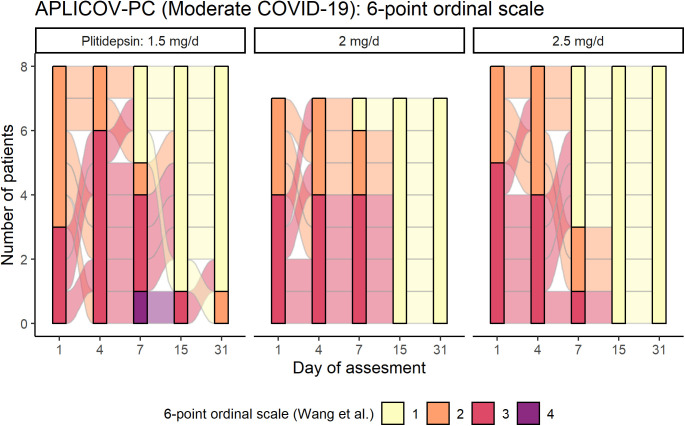
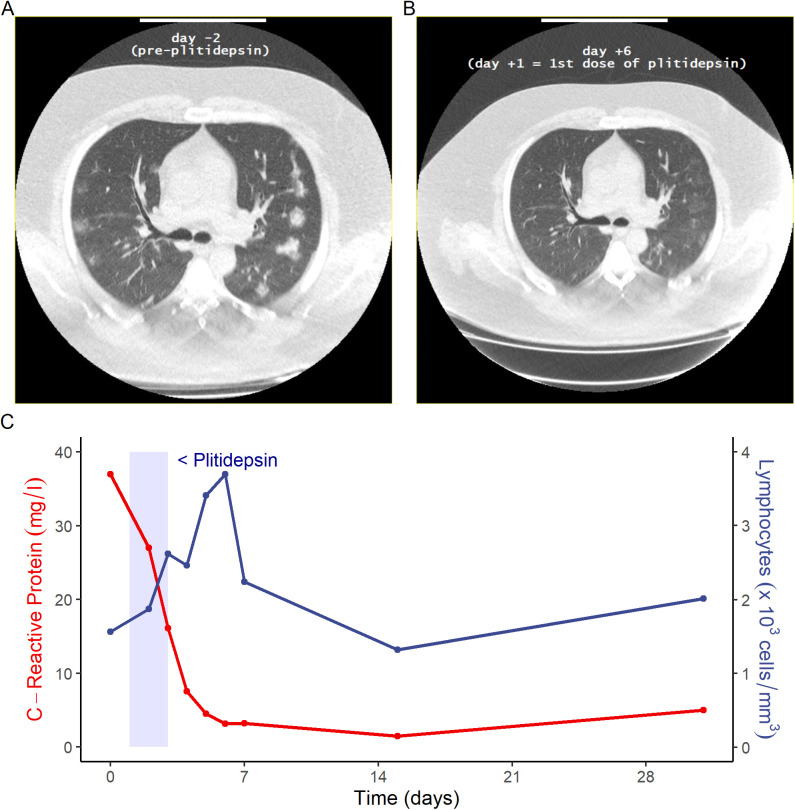
Plitidepsin, a marine-derived cyclic-peptide, inhibits SARS-CoV-2 replication at nanomolar concentrations by targeting the host protein eukaryotic translation elongation factor 1A. Here, we show that plitidepsin distributes preferentially to lung over plasma, with similar potency against across several SARS-CoV-2 variants in preclinical studies. Simultaneously, in this randomized, parallel, open-label, proof-of-concept study (NCT04382066) conducted in 10 Spanish hospitals between May and November 2020, 46 adult hospitalized patients with confirmed SARS-CoV-2 infection received either 1.5 mg (n = 15), 2.0 mg (n = 16), or 2.5 mg (n = 15) plitidepsin once daily for 3 d. The primary objective was safety; viral load kinetics, mortality, need for increased respiratory support, and dose selection were secondary end points. One patient withdrew consent before starting procedures; 45 initiated treatment; one withdrew because of hypersensitivity. Two Grade 3 treatment-related adverse events were observed (hypersensitivity and diarrhea). Treatment-related adverse events affecting more than 5% of patients were nausea (42.2%), vomiting (15.6%), and diarrhea (6.7%). Mean viral load reductions from baseline were 1.35, 2.35, 3.25, and 3.85 log10 at days 4, 7, 15, and 31. Nonmechanical invasive ventilation was required in 8 of 44 evaluable patients (16.0%); six patients required intensive care support (13.6%), and three patients (6.7%) died (COVID-19-related). Plitidepsin has a favorable safety profile in patients with COVID-19.
© 2022 Varona et al.
Conflict of interest statement
V Estrada has received personal fees from Janssen, Gilead, and ViiV and grants from MSD. R Paredes has participated in Advisory Boards from Gilead, MSD, ViiV Healthcare, and Theratechnologies. M Torralba has received consulting fees as a member of Advisory Committee and honoraria and speaking fees from Gilead, Janssen, MSD, and ViiV Companies. J Fortún has participated in scientific events and received consulting or speaking fees or oral presentations from Pfizer, Gilead, MSD, Astellas, Novartis, and Roche. J Ancochea has received fees for scientific consulting and/or speaking from Actelion, Air Liquide, Almirall, AstraZeneca, Boehringer Ingelheim, Carburos Médica, Chiesi, Faes Farma, Ferrer, GlaxoSmithKline, InterMune, Linde Healthcare, Menarini, MSD, Mundipharma, Novartis, Pfizer, Roche, Rovi, Sandoz, Takeda, and Teva. I Sola, S Zúñiga, and L Enjuanes hold a Technology Support contract with Pharmamar. N Izquierdo-Useros is inventor of a patent of Plitidepsin (EP20382821.5). The Krogan Laboratory has received research support from Vir Biotechnology and F Hoffmann-La Roche. NJ Krogan has consulting agreements with Maze Therapeutics and Interline Therapeutics, and is a shareholder of Tenaya Therapeutics. JM Fernández-Sousa is President and Founder of Pharmamar, SA (Madrid, Spain). JM Jimeno holds stocks of Pangaea Oncology, has a non-remunerated role in the Scientific Advisory Board and holds stocks of Phosplatin Therapeutics, and is a full-time employee of Pharmamar, SA (Madrid, Spain).The A García-Sastre laboratory has received research support from Pfizer, Senhwa Biosciences, Kenall Manufacturing, Avimex, Johnson & Johnson, Dynavax, 7Hills Pharma, Pharmamar, ImmunityBio, Accurius, and Nanocomposix. A García-Sastre has consulting agreements for the following companies involving cash and/or stock: Vivaldi Biosciences, Contrafect, 7Hills Pharma, Avimex, Vaxalto, Pagoda, Accurius, Esperovax, Farmak, and Pfizer. A García-Sastre is inventor on patents and patent application on the use of antivirals for the treatment of virus infections, owned by the Icahn School of Medicine at Mount Sinai, New York. A patent application based on this work has been filed (EP20382821.5). JA Lopez-Martin, S Fudio, MJ Pontes, B de Rivas, A Nieto, J Gómez, P Girón de Velasco, P Avilés, R Lubomirov, A Belgrano, and B Sopesén are employees and shareholders of Pharmamar, SA (Madrid, Spain). JA Lopez-Martin is a co-inventor of a patent for plitidepsin (WO2008135793A1). JM Jimeno is a co-inventor on a patent for didmenin (WO99/42125) and on patents for aplidine (WO03/033013 and WO 2004/080421).
Figures




Update of
-
Plitidepsin has a positive therapeutic index in adult patients with COVID-19 requiring hospitalization.medRxiv [Preprint]. 2021 May 25:2021.05.25.21257505. doi: 10.1101/2021.05.25.21257505. medRxiv. 2021. Update in: Life Sci Alliance. 2022 Jan 10;5(4):e202101200. doi: 10.26508/lsa.202101200. PMID: 34075384 Free PMC article. Updated. Preprint.
References
-
- World Health Organization (2021) COVID-19 Dashboard. Available online https://covid19.who.int/. Accessed 13 December 2021.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous