

Microwave versus radiofrequency ablation for the treatment of liver malignancies: a randomized controlled phase 2 trial
- PMID: 35013377
- PMCID: PMC8748896
- DOI: 10.1038/s41598-021-03802-x
Microwave versus radiofrequency ablation for the treatment of liver malignancies: a randomized controlled phase 2 trial
Abstract
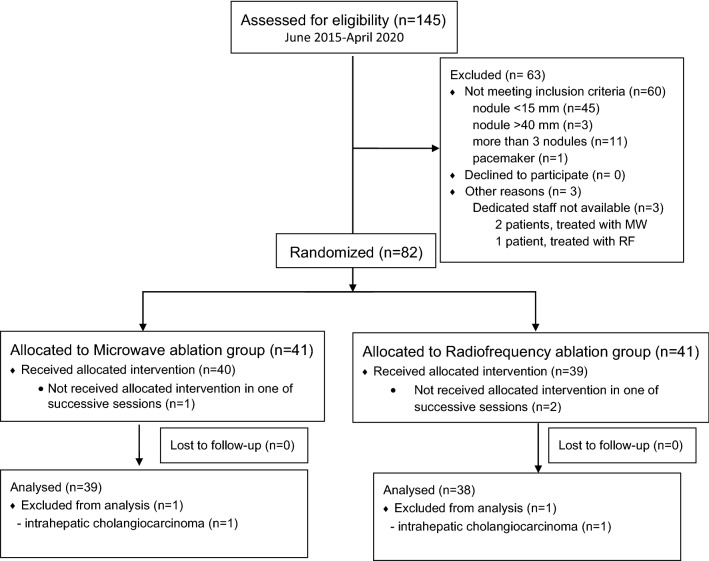
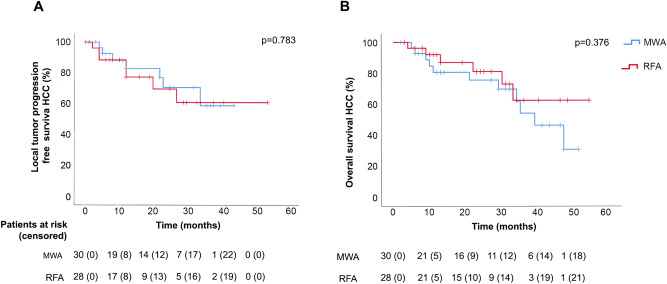
Microwave (MWA) and radiofrequency ablation (RFA) are main ablative techniques for hepatocellular carcinoma (HCC) and colorectal liver metastasis (MT). This randomized phase 2 clinical trial compares the effectiveness of MWA and RFA as well as morphology of corresponding ablation zones. HCC and MT patients with 1.5-4 cm tumors, suitable for ablation, were randomized into MWA or RFA Groups. The primary endpoint was short-to-long diameter ratio of ablation zone (SLR). Primary technical success (TS) and a cumulative local tumor progression (LTP) after a median 2-year follow-up were compared. Between June 2015 and April 2020, 82 patients were randomly assigned (41 patients per group). For the per-protocol analysis, five patients were excluded. MWA created larger ablation zones than RFA (p = 0.036) although without differences in SLR (0.5 for both groups, p = 0.229). The TS was achieved in 98% (46/47) and 90% (45/50) (p = 0.108), and LTP was observed in 21% (10/47) vs. 12% (6/50) (OR 1.9 [95% CI 0.66-5.3], p = 0.238) of tumors in MWA vs. RFA Group, respectively. Major complications were found in 5 cases (11%) vs. 2 cases (4%), without statistical significance. MWA and RFA show similar SLR, effectiveness and safety in liver tumors between 1.5 and 4 cm.
© 2022. The Author(s).
Conflict of interest statement
A.R. and F.B. report non-financial support from HS Hospital Service (Rome, Italy). F.B. is inventor of a patent related with the applicator used in RFA Group (licensed to Apeiron Medical, Valencia, Spain). F.B. also reports personal lectures fees from HS Hospital service and personal lectures fees from Apeiron Medical. The other authors do not have any conflict of interest to disclose.
Figures
References
-
- Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet. 2018;391:1301–1314. - PubMed
-
- Nault JC, Sutter O, Nahon P, Ganne-Carrié N, Séror O. Percutaneous treatment of hepatocellular carcinoma: State of the art and innovations. J. Hepatol. 2018;68:783–797. - PubMed
-
- Van Cutsem E, et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann. Oncol. 2016;27:1386–1422. - PubMed
-
- Sacks D, McClenny TE, Cardella JF, Lewis CA. Society of Interventional Radiology clinical practice guidelines. J. Vasc. Interv. Radiol. 2003;14:S199–202. - PubMed
Publication types
MeSH terms
Grants and funding
- FIS - PI12/00799/Spanish Government
- FIS - PI12/00799/Spanish Government
- FIS - PI12/00799/Spanish Government
- FIS - PI12/00799/Spanish Government
- FIS - PI12/00799/Spanish Government
- FIS - PI12/00799/Spanish Government
- FIS - PI12/00799/Spanish Government
- FIS - PI12/00799/Spanish Government
- FIS - PI12/00799/Spanish Government
- FIS - PI12/00799/Spanish Government
- FIS - PI12/00799/Spanish Government
- FIS - PI12/00799/Spanish Government
- FIS - PI12/00799/Spanish Government
- FIS - PI12/00799/Spanish Government
- FIS - PI12/00799/Spanish Government
- FIS - PI12/00799/Spanish Government
- FIS - PI12/00799/Spanish Government
- FIS - PI12/00799/Spanish Government
- FIS - PI12/00799/Spanish Government
- FIS - PI12/00799/Spanish Government
- FIS - PI12/00799/Spanish Government
- FIS - PI12/00799/Spanish Government
- RTI2018-094357-B-C21/Spanish Ministerio de Ciencia, Innovación y Universidades under "Programa Estatal de I+D+i Orientada a los Retos de la Sociedad"
- RTI2018-094357-B-C21/Spanish Ministerio de Ciencia, Innovación y Universidades under "Programa Estatal de I+D+i Orientada a los Retos de la Sociedad"
- RTI2018-094357-B-C21/Spanish Ministerio de Ciencia, Innovación y Universidades under "Programa Estatal de I+D+i Orientada a los Retos de la Sociedad"
- RTI2018-094357-B-C21/Spanish Ministerio de Ciencia, Innovación y Universidades under "Programa Estatal de I+D+i Orientada a los Retos de la Sociedad"
- RTI2018-094357-B-C21/Spanish Ministerio de Ciencia, Innovación y Universidades under "Programa Estatal de I+D+i Orientada a los Retos de la Sociedad"
- RTI2018-094357-B-C21/Spanish Ministerio de Ciencia, Innovación y Universidades under "Programa Estatal de I+D+i Orientada a los Retos de la Sociedad"
- RTI2018-094357-B-C21/Spanish Ministerio de Ciencia, Innovación y Universidades under "Programa Estatal de I+D+i Orientada a los Retos de la Sociedad"
- RTI2018-094357-B-C21/Spanish Ministerio de Ciencia, Innovación y Universidades under "Programa Estatal de I+D+i Orientada a los Retos de la Sociedad"
- RTI2018-094357-B-C21/Spanish Ministerio de Ciencia, Innovación y Universidades under "Programa Estatal de I+D+i Orientada a los Retos de la Sociedad"
- RTI2018-094357-B-C21/Spanish Ministerio de Ciencia, Innovación y Universidades under "Programa Estatal de I+D+i Orientada a los Retos de la Sociedad"
- RTI2018-094357-B-C21/Spanish Ministerio de Ciencia, Innovación y Universidades under "Programa Estatal de I+D+i Orientada a los Retos de la Sociedad"
- RTI2018-094357-B-C21/Spanish Ministerio de Ciencia, Innovación y Universidades under "Programa Estatal de I+D+i Orientada a los Retos de la Sociedad"
- RTI2018-094357-B-C21/Spanish Ministerio de Ciencia, Innovación y Universidades under "Programa Estatal de I+D+i Orientada a los Retos de la Sociedad"
- RTI2018-094357-B-C21/Spanish Ministerio de Ciencia, Innovación y Universidades under "Programa Estatal de I+D+i Orientada a los Retos de la Sociedad"
- RTI2018-094357-B-C21/Spanish Ministerio de Ciencia, Innovación y Universidades under "Programa Estatal de I+D+i Orientada a los Retos de la Sociedad"
- RTI2018-094357-B-C21/Spanish Ministerio de Ciencia, Innovación y Universidades under "Programa Estatal de I+D+i Orientada a los Retos de la Sociedad"
- RTI2018-094357-B-C21/Spanish Ministerio de Ciencia, Innovación y Universidades under "Programa Estatal de I+D+i Orientada a los Retos de la Sociedad"
- RTI2018-094357-B-C21/Spanish Ministerio de Ciencia, Innovación y Universidades under "Programa Estatal de I+D+i Orientada a los Retos de la Sociedad"
- RTI2018-094357-B-C21/Spanish Ministerio de Ciencia, Innovación y Universidades under "Programa Estatal de I+D+i Orientada a los Retos de la Sociedad"
- RTI2018-094357-B-C21/Spanish Ministerio de Ciencia, Innovación y Universidades under "Programa Estatal de I+D+i Orientada a los Retos de la Sociedad"
- RTI2018-094357-B-C21/Spanish Ministerio de Ciencia, Innovación y Universidades under "Programa Estatal de I+D+i Orientada a los Retos de la Sociedad"
- RTI2018-094357-B-C21/Spanish Ministerio de Ciencia, Innovación y Universidades under "Programa Estatal de I+D+i Orientada a los Retos de la Sociedad"
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
