

Tissue Engineered Neurovascularization Strategies for Craniofacial Tissue Regeneration
- PMID: 35014834
- PMCID: PMC9016342
- DOI: 10.1021/acsabm.1c00979
Tissue Engineered Neurovascularization Strategies for Craniofacial Tissue Regeneration
Abstract
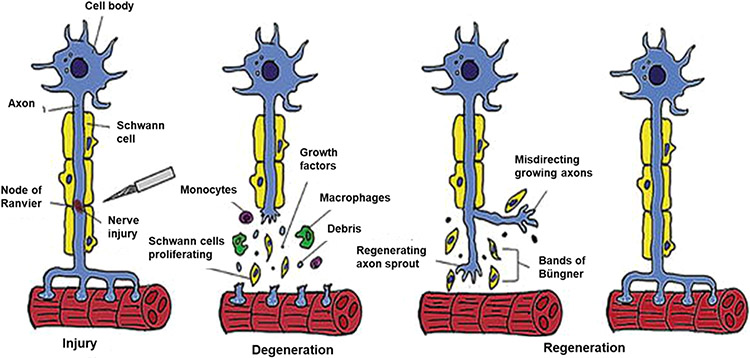
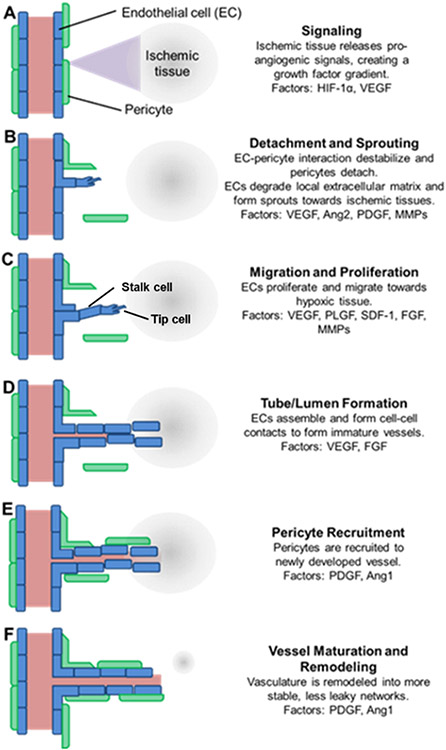
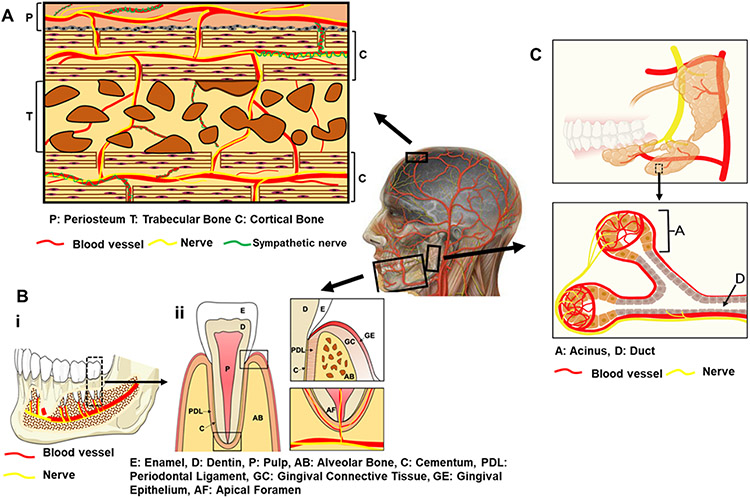
Craniofacial tissue injuries, diseases, and defects, including those within bone, dental, and periodontal tissues and salivary glands, impact an estimated 1 billion patients globally. Craniofacial tissue dysfunction significantly reduces quality of life, and successful repair of damaged tissues remains a significant challenge. Blood vessels and nerves are colocalized within craniofacial tissues and act synergistically during tissue regeneration. Therefore, the success of craniofacial regenerative approaches is predicated on successful recruitment, regeneration, or integration of both vascularization and innervation. Tissue engineering strategies have been widely used to encourage vascularization and, more recently, to improve innervation through host tissue recruitment or prevascularization/innervation of engineered tissues. However, current scaffold designs and cell or growth factor delivery approaches often fail to synergistically coordinate both vascularization and innervation to orchestrate successful tissue regeneration. Additionally, tissue engineering approaches are typically investigated separately for vascularization and innervation. Since both tissues act in concert to improve craniofacial tissue regeneration outcomes, a revised approach for development of engineered materials is required. This review aims to provide an overview of neurovascularization in craniofacial tissues and strategies to target either process thus far. Finally, key design principles are described for engineering approaches that will support both vascularization and innervation for successful craniofacial tissue regeneration.
Keywords: biomaterial design; cell therapy; craniofacial tissue; engineered tissue regeneration; growth factor; hydrogel; neurovascularization.
Figures
References
-
- Warren SM; Fong KD; Chen CM; Loboa EG; Cowan CM; Lorenz HP; Longaker MT Tools and techniques for craniofacial tissue engineering. Tissue Eng. 2003, 9 (2), 187–200. - PubMed
-
- Petrovic V; Zivkovic P; Petrovic D; Stefanovic V Craniofacial bone tissue engineering. Oral surgery, oral medicine, oral pathology and oral radiology 2012, 114 (3), No. e1. - PubMed
-
- Ozdemir D Dental caries: the most common disease worldwide and preventive strategies. Int. J. Biol 2013, 5 (4), 55.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources