

Pregnancy Complications and Risk of Cardiovascular Disease Later in Life: A Nationwide Cohort Study
- PMID: 35014876
- PMCID: PMC9238523
- DOI: 10.1161/JAHA.121.023079
Pregnancy Complications and Risk of Cardiovascular Disease Later in Life: A Nationwide Cohort Study
Abstract
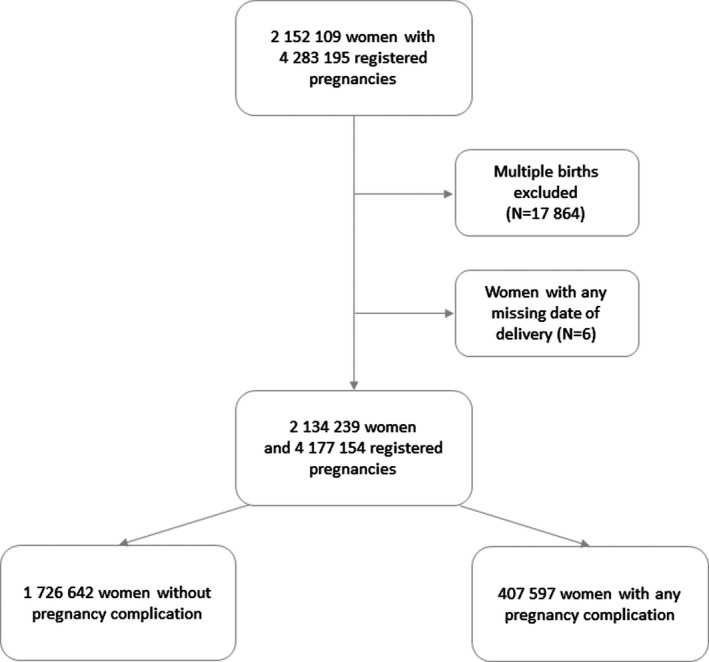
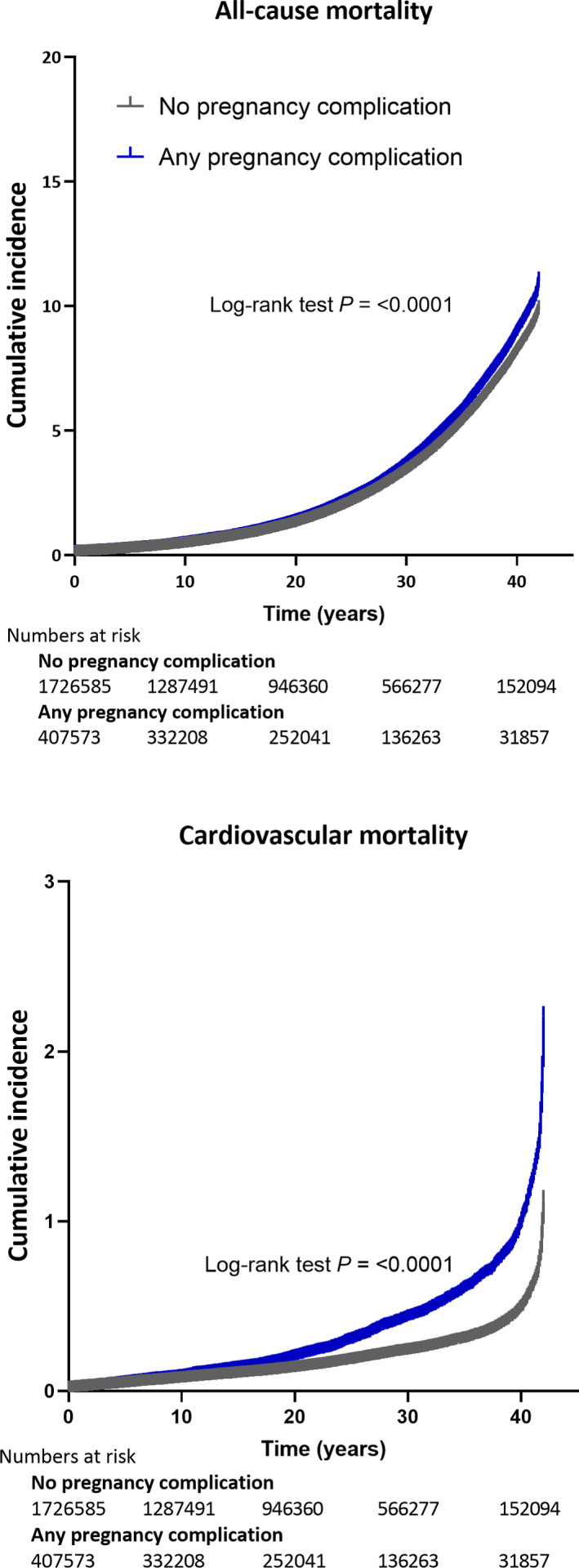
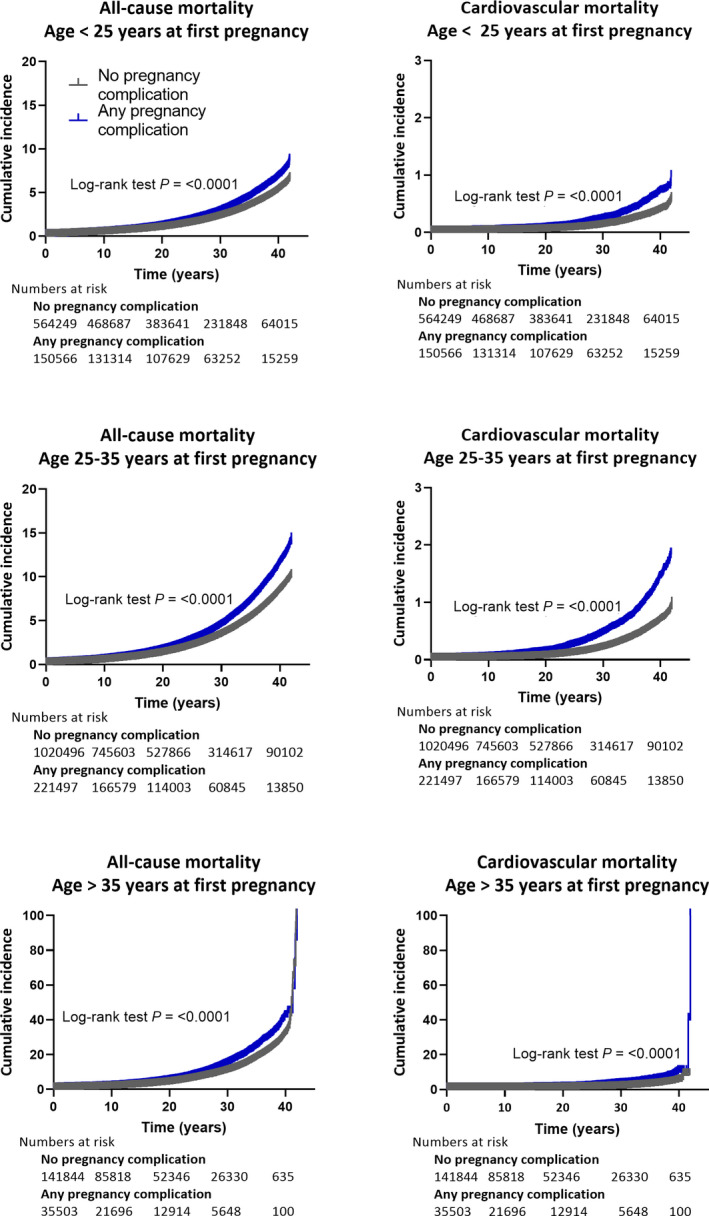
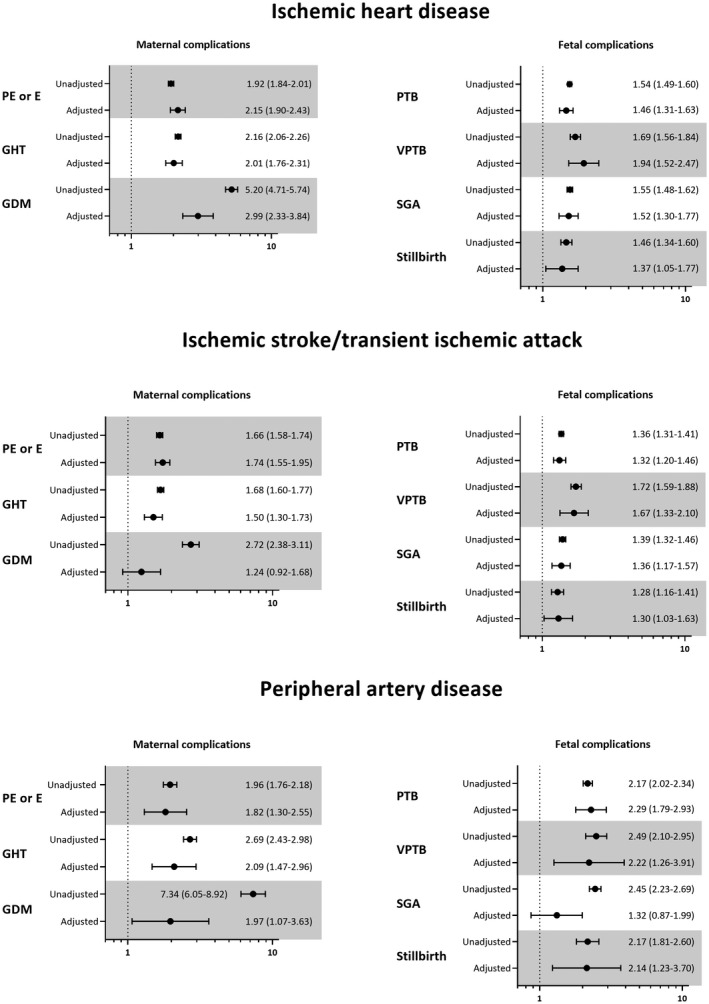
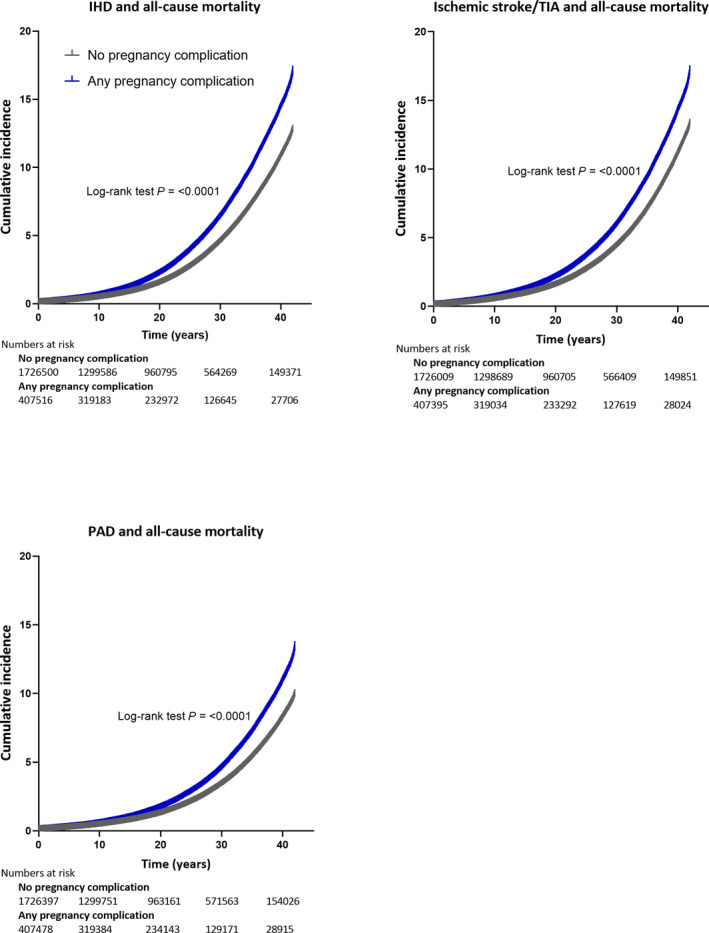
Background The aim of this study was to investigate the associations between pregnancy complications and cardiovascular mortality and hospitalizations of cardiovascular disease (CVD) after adjustment for major confounding. Methods and Results In a nationwide register-based cohort study, women with singleton births between 1973 and 2014 were included from the Swedish Medical Birth Register. Outcomes of mortality and hospitalizations of CVD were collected from the Cause of Death Register and the National Inpatient Register. The cohort was followed from the date of the first delivery until death or end of follow-up, whichever occurred first. The pregnancy complications studied were preeclampsia or eclampsia, gestational hypertension, gestational diabetes, preterm birth, small for gestational age, and stillbirth. Among the 2 134 239 women (mean age at first pregnancy, 27.0 [SD, 5.1] and mean parity 1.96 [SD, 0.9]), 19.1% (N=407 597) had 1 of the studied pregnancy complications. All pregnancy complications were associated with all-cause and cardiovascular mortality and hospitalization for CVD (ischemic heart disease, ischemic stroke, and peripheral artery disease) after adjustment for major confounding in a Cox proportional hazard regression model. The adjusted hazard ratio for cardiovascular mortality was 1.84 (95% CI, 1.38-2.44) for preterm birth and 3.14 (95% CI, 1.81-5.44) for stillbirth. Conclusions In this large cohort study, pregnancy complications were associated with all-cause mortality, cardiovascular mortality, and hospitalizations for CVD, also after adjusting for confounding, including overweight, smoking, and comorbidities. The study highlights that less established pregnancy complications such as preterm birth and stillbirth are also associated with cardiovascular mortality and CVD.
Keywords: cardiovascular disease; ischemic heart disease; ischemic stroke; peripheral artery disease; pregnancy complications.
Figures
References
-
- Mosca L, Benjamin EJ, Berra K, Bezanson JL, Dolor RJ, Lloyd‐Jones DM, Newby LK, Piña IL, Roger VL, Shaw LJ, et al. Effectiveness‐based guidelines for the prevention of cardiovascular disease in women – 2011 update: a guideline from the American Heart Association. Circulation. 2011;123:1243–1262. doi: 10.1161/CIR.0b013e31820faaf8 - DOI - PMC - PubMed
-
- Piepoli MF, Hoes AW, Agewall S, Albus C, Brotons C, Catapano AL, Cooney M‐T, Corrà U, Cosyns B, Deaton C, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J. 2016;37:2315–2381. doi: 10.1093/eurheartj/ehw106 - DOI - PMC - PubMed
-
- Bellamy L, Casas JP, Hingorani AD, Williams DJ. Pre‐eclampsia and risk of cardiovascular disease and cancer in later life: systematic review and meta‐analysis. Meta‐Analysis Research Support, Non‐U.S. Gov’t Review. BMJ. 2007;335(7627):974. doi: 10.1136/bmj.39335.385301.BE - DOI - PMC - PubMed
-
- Mongraw‐Chaffin ML, Cirillo PM, Cohn BA. Preeclampsia and cardiovascular disease death: prospective evidence from the child health and development studies cohort. Comparative Study Research Support, N.I.H., Extramural. Hypertension. 2010;56:166–171. doi: 10.1161/HYPERTENSIONAHA.110.150078 - DOI - PMC - PubMed
-
- Skjaerven R, Wilcox AJ, Klungsoyr K, Irgens LM, Vikse BE, Vatten LJ, Lie RT. Cardiovascular mortality after pre‐eclampsia in one child mothers: prospective, population based cohort study. Comparative Study Research Support, N.I.H., Intramural Research Support, Non‐U.S. Gov’t. BMJ. 2012;345:e7677. doi: 10.1136/bmj.e7677 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
