

The efficacy of psychotherapies and pharmacotherapies for mental disorders in adults: an umbrella review and meta-analytic evaluation of recent meta-analyses
- PMID: 35015359
- PMCID: PMC8751557
- DOI: 10.1002/wps.20941
The efficacy of psychotherapies and pharmacotherapies for mental disorders in adults: an umbrella review and meta-analytic evaluation of recent meta-analyses
Abstract
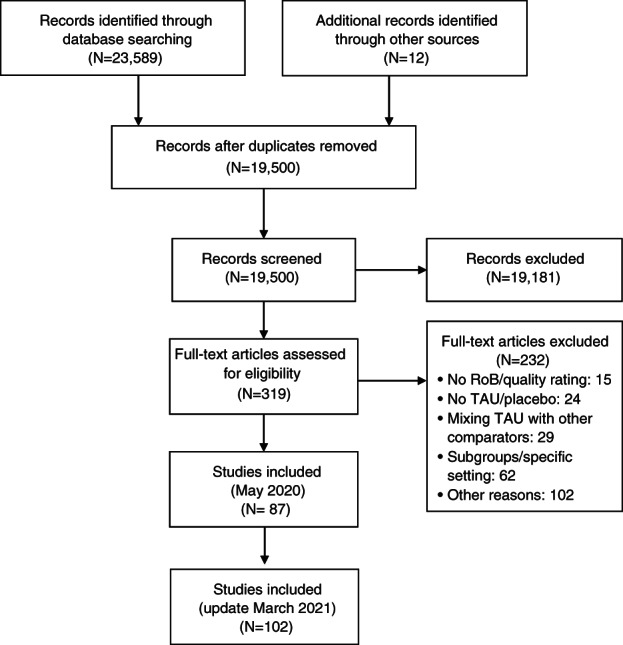
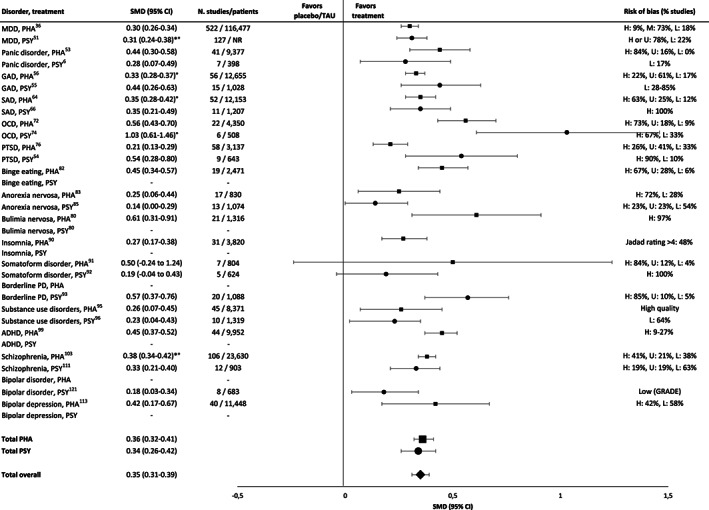
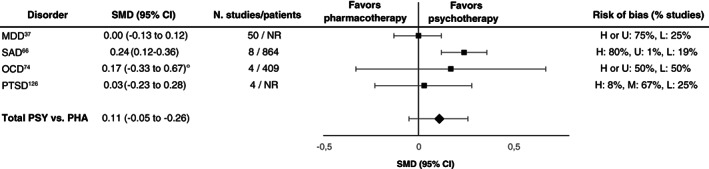
Mental disorders represent a worldwide public health concern. Psychotherapies and pharmacotherapies are recommended as first line treatments. However, evidence has emerged that their efficacy may be overestimated, due to a variety of shortcomings in clinical trials (e.g., publication bias, weak control conditions such as waiting list). We performed an umbrella review of recent meta-analyses of randomized controlled trials (RCTs) of psychotherapies and pharmacotherapies for the main mental disorders in adults. We selected meta-analyses that formally assessed risk of bias or quality of studies, excluded weak comparators, and used effect sizes for target symptoms as primary outcome. We searched PubMed and PsycINFO and individual records of the Cochrane Library for meta-analyses published between January 2014 and March 2021 comparing psychotherapies or pharmacotherapies with placebo or treatment-as-usual (TAU), or psychotherapies vs. pharmacotherapies head-to-head, or the combination of psychotherapy with pharmacotherapy to either monotherapy. One hundred and two meta-analyses, encompassing 3,782 RCTs and 650,514 patients, were included, covering depressive disorders, anxiety disorders, post-traumatic stress disorder, obsessive-compulsive disorder, somatoform disorders, eating disorders, attention-deficit/hyperactivity disorder, substance use disorders, insomnia, schizophrenia spectrum disorders, and bipolar disorder. Across disorders and treatments, the majority of effect sizes for target symptoms were small. A random effect meta-analytic evaluation of the effect sizes reported by the largest meta-analyses per disorder yielded a standardized mean difference (SMD) of 0.34 (95% CI: 0.26-0.42) for psychotherapies and 0.36 (95% CI: 0.32-0.41) for pharmacotherapies compared with placebo or TAU. The SMD for head-to-head comparisons of psychotherapies vs. pharmacotherapies was 0.11 (95% CI: -0.05 to 0.26). The SMD for the combined treatment compared with either monotherapy was 0.31 (95% CI: 0.19-0.44). Risk of bias was often high. After more than half a century of research, thousands of RCTs and millions of invested funds, the effect sizes of psychotherapies and pharmacotherapies for mental disorders are limited, suggesting a ceiling effect for treatment research as presently conducted. A paradigm shift in research seems to be required to achieve further progress.
Keywords: Psychotherapies; effect sizes; mental disorders; meta-analyses; meta-analytic evaluation; pharmacotherapies; randomized controlled trials.
© 2022 World Psychiatric Association.
Figures
References
-
- Vigo D, Thornicroft G, Atun R. Estimating the true global burden of mental illness. Lancet Psychiatry 2016;3:171‐8. - PubMed
-
- Smith K. Trillion‐dollar brain drain – enormous costs of mental health problems in Europe not matched by research investment. Nature 2011;478:15. - PubMed
-
- Nathan PE, Gorman JM. A guide to treatments that work, 4th ed. New York: Oxford University Press, 2015.
-
- National Institute for Health and Care Excellence . Mental health and behavioural conditions. https://www.nice.org.uk.
-
- Cuijpers P, Karyotaki E, Weitz E et al. The effects of psychotherapies for major depression in adults on remission, recovery and improvement: a meta‐analysis. J Affect Disord 2014;159:118‐26. - PubMed
LinkOut - more resources
Full Text Sources
Medical
