

Daily Exposure to Mild Intermittent Hypoxia Reduces Blood Pressure in Male Patients with Obstructive Sleep Apnea and Hypertension
- PMID: 35015980
- PMCID: PMC9838631
- DOI: 10.1164/rccm.202108-1808OC
Daily Exposure to Mild Intermittent Hypoxia Reduces Blood Pressure in Male Patients with Obstructive Sleep Apnea and Hypertension
Abstract
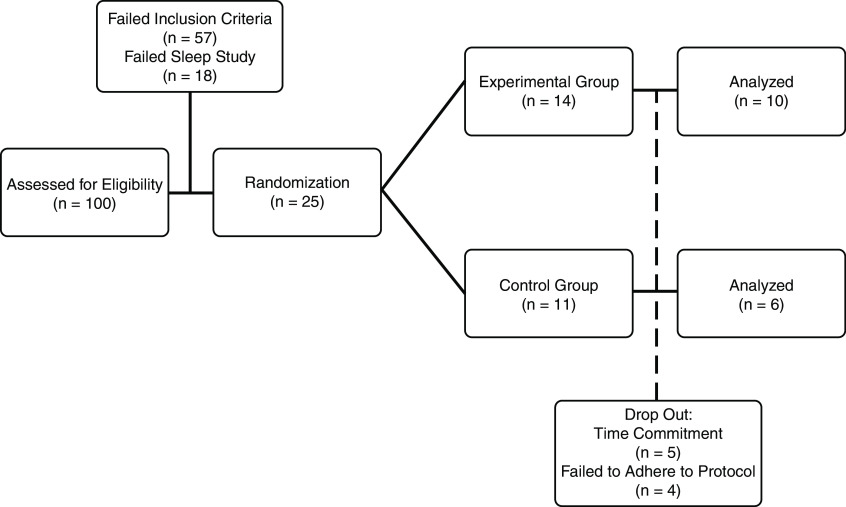
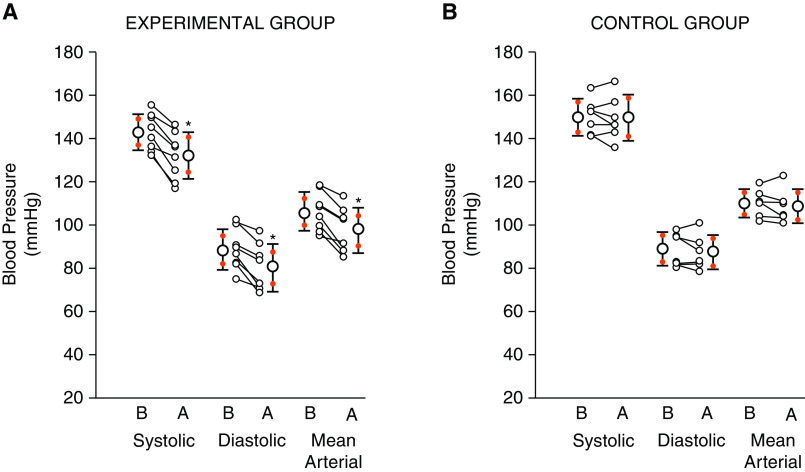
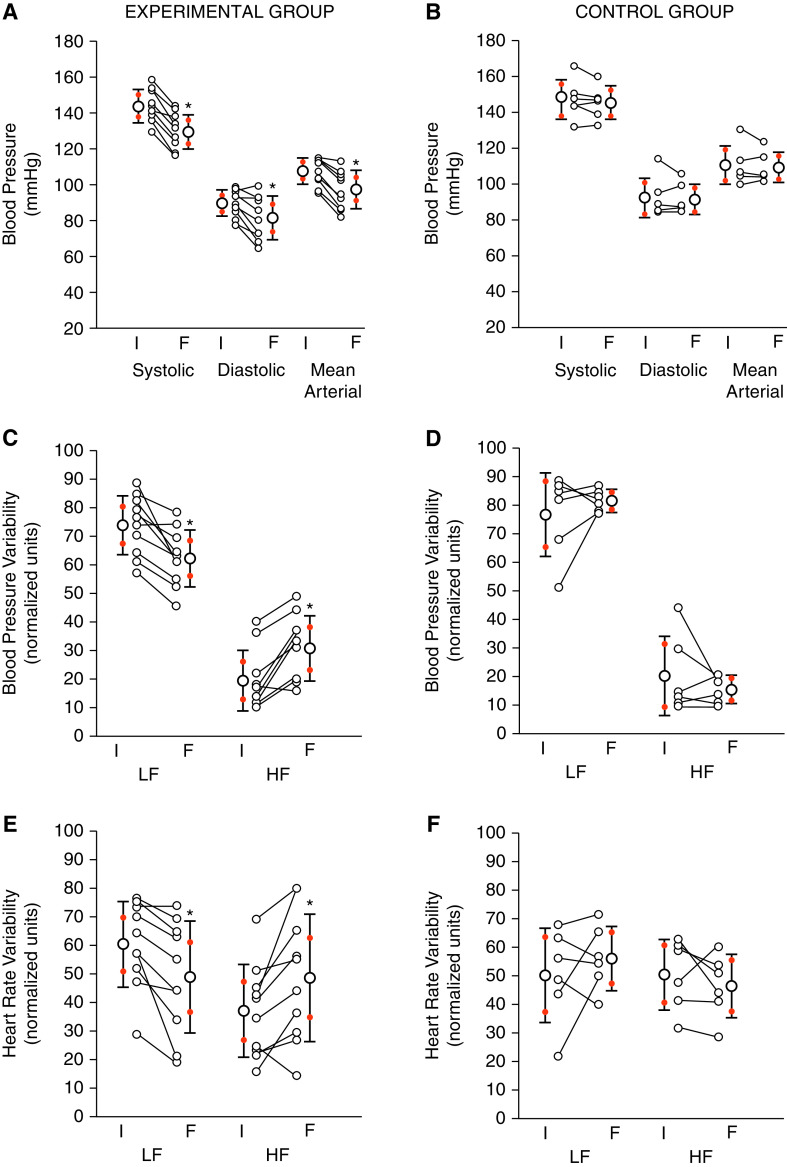
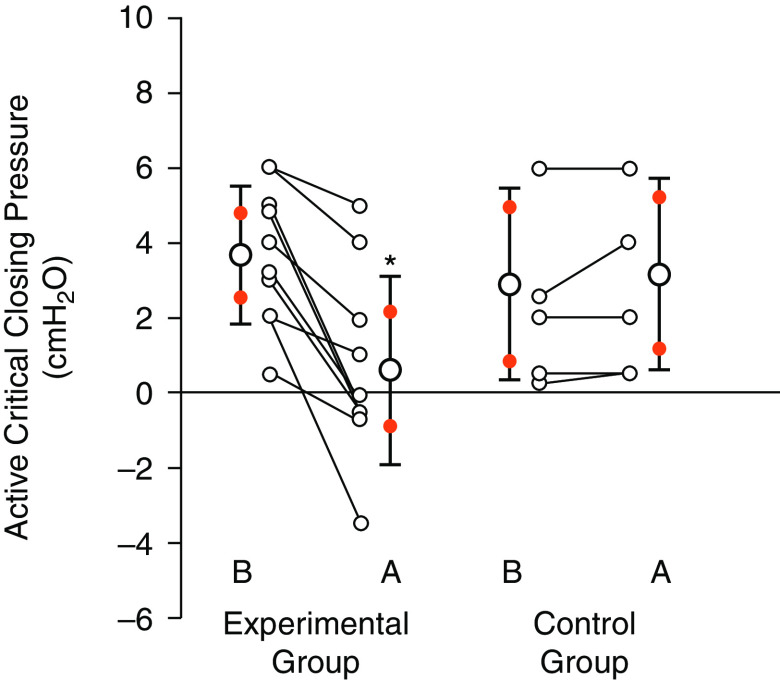
Rationale: Daily exposure to mild intermittent hypoxia (MIH) may elicit beneficial cardiovascular outcomes. Objectives: To determine the effect of 15 days of MIH and in-home continuous positive airway pressure treatment on blood pressure in participants with obstructive sleep apnea and hypertension. Methods: We administered MIH during wakefulness 5 days/week for 3 weeks. The protocol consisted of twelve 2-minute bouts of hypoxia interspersed with 2 minutes of normoxia. End-tidal carbon dioxide was maintained 2 mm Hg above baseline values throughout the protocol. Control participants were exposed to a sham protocol (i.e., compressed air). All participants were treated with continuous positive airway pressure over the 3-week period. Results are mean ± SD. Measurements and Main Results: Sixteen male participants completed the study (experimental n = 10; control n = 6). Systolic blood pressure at rest during wakefulness over 24 hours was reduced after 15 days of MIH (142.9 ± 8.6 vs. 132.0 ± 10.7 mm Hg; P < 0.001), but not following the sham protocol (149.9 ± 8.6 vs. 149.7 ± 10.8 mm Hg; P = 0.915). Thus, the reduction in blood pressure from baseline was greater in the experimental group compared with control (-10.91 ± 4.1 vs. -0.17 ± 3.6 mm Hg; P = 0.003). Modifications in blood pressure were accompanied by increased parasympathetic and reduced sympathetic activity in the experimental group, as estimated by blood pressure and heart rate variability analysis. No detrimental neurocognitive and metabolic outcomes were evident following MIH. Conclusions: MIH elicits beneficial cardiovascular and autonomic outcomes in males with OSA and concurrent hypertension. Clinical trial registered with www.clinicaltrials.gov (NCT03736382).
Keywords: continuous positive airway pressure; hypertension; intermittent hypoxia; obstructive sleep apnea.
Figures
Comment in
-
Hypoxia and Sleep-disordered Breathing: Friend or Foe?Am J Respir Crit Care Med. 2022 Apr 15;205(8):869-872. doi: 10.1164/rccm.202201-0113ED. Am J Respir Crit Care Med. 2022. PMID: 35196476 Free PMC article. No abstract available.
-
Reply to Chen et al.: Mild Intermittent Hypoxia: A New Treatment Approach for Patients with Obstructive Sleep Apnea and Hypertension.Am J Respir Crit Care Med. 2022 Jul 1;206(1):123-124. doi: 10.1164/rccm.202202-0228LE. Am J Respir Crit Care Med. 2022. PMID: 35476606 Free PMC article. No abstract available.
-
Mild Intermittent Hypoxia: A New Treatment Approach for Patients with Obstructive Sleep Apnea and Hypertension.Am J Respir Crit Care Med. 2022 Jul 1;206(1):122-123. doi: 10.1164/rccm.202201-0134LE. Am J Respir Crit Care Med. 2022. PMID: 35476716 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
