

Effects of virtual reality-based motor control training on inflammation, oxidative stress, neuroplasticity and upper limb motor function in patients with chronic stroke: a randomized controlled trial
- PMID: 35016629
- PMCID: PMC8751278
- DOI: 10.1186/s12883-021-02547-4
Effects of virtual reality-based motor control training on inflammation, oxidative stress, neuroplasticity and upper limb motor function in patients with chronic stroke: a randomized controlled trial
Abstract
Background: Immersive virtual reality (VR)-based motor control training (VRT) is an innovative approach to improve motor function in patients with stroke. Currently, outcome measures for immersive VRT mainly focus on motor function. However, serum biomarkers help detect precise and subtle physiological changes. Therefore, this study aimed to identify the effects of immersive VRT on inflammation, oxidative stress, neuroplasticity and upper limb motor function in stroke patients.
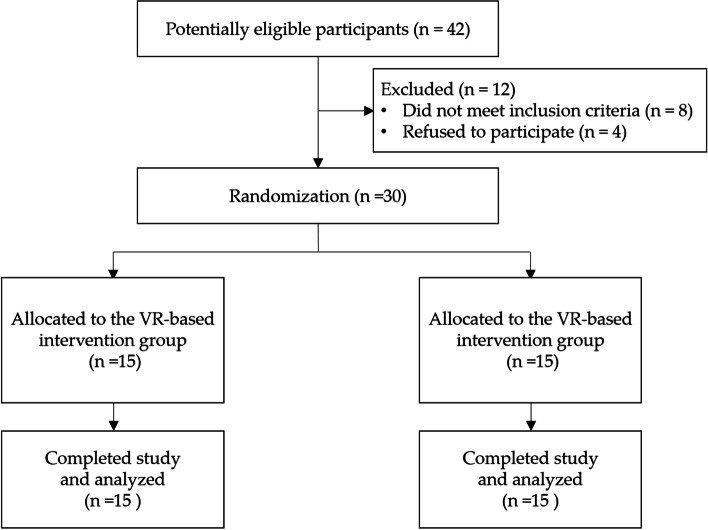
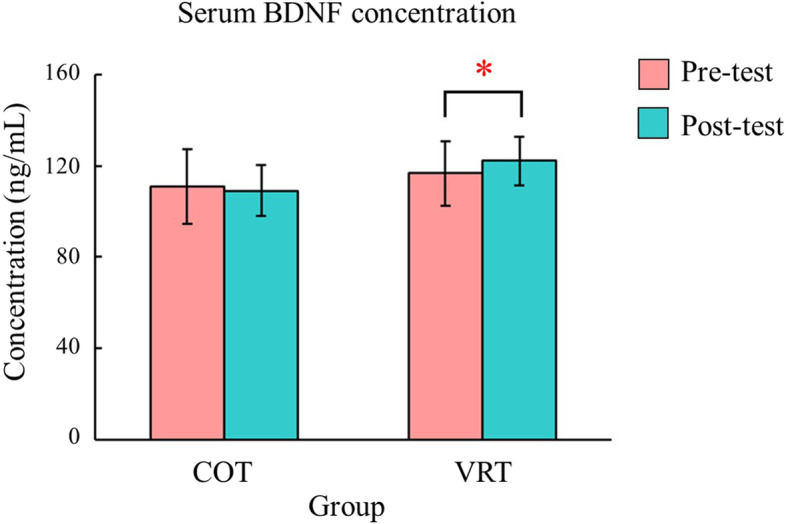
Methods: Thirty patients with chronic stroke were randomized to the VRT or conventional occupational therapy (COT) groups. Serum biomarkers including interleukin 6 (IL-6), intracellular adhesion molecule 1 (ICAM-1), heme oxygenase 1 (HO-1), 8-hydroxy-2-deoxyguanosine (8-OHdG), and brain-derived neurotrophic factor (BDNF) were assessed to reflect inflammation, oxidative stress and neuroplasticity. Clinical assessments including active range of motion of the upper limb and the Fugl-Meyer Assessment for upper extremity (FMA-UE) were also used. Two-way mixed analyses of variance (ANOVAs) were used to examine the effects of the intervention (VRT and COT) and time on serum biomarkers and upper limb motor function.
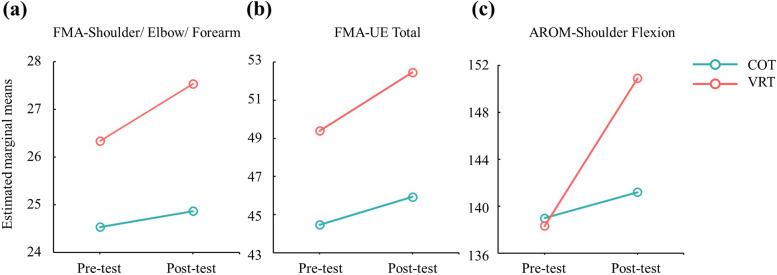
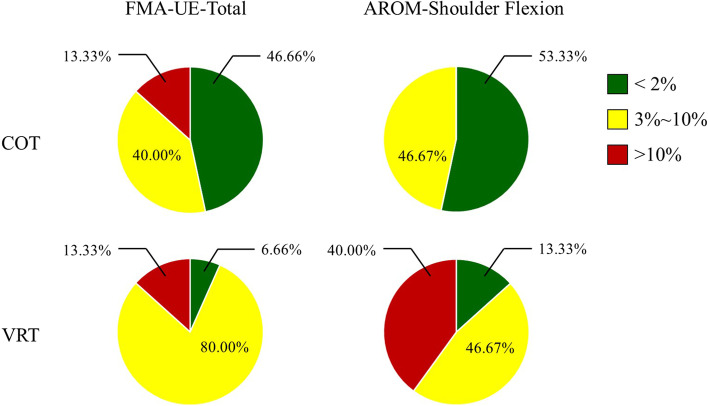
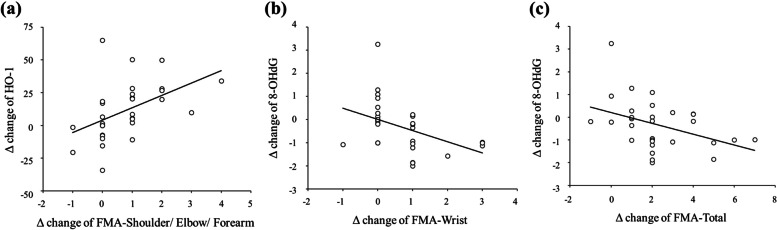
Results: We found significant time effects in serum IL-6 (p = 0.010), HO-1 (p = 0.002), 8-OHdG (p = 0.045), and all items/subscales of the clinical assessments (ps < 0.05), except FMA-UE-Coordination/Speed (p = 0.055). However, significant group effects existed only in items of the AROM-Elbow Extension (p = 0.007) and AROM-Forearm Pronation (p = 0.048). Moreover, significant interactions between time and group existed in item/subscales of FMA-UE-Shoulder/Elbow/Forearm (p = 0.004), FMA-UE-Total score (p = 0.008), and AROM-Shoulder Flexion (p = 0.001).
Conclusion: This was the first study to combine the effectiveness of immersive VRT using serum biomarkers as outcome measures. Our study demonstrated promising results that support the further application of commercial and immersive VR technologies in patients with chronic stroke.
Keywords: 8-hydroxydeoxyguanosine (8-OHdG); Brain-derived neurotrophic factor (BDNF); Heme oxygenase-1 (HO-1); Inflammation; Neuroplasticity; Oxidative stress; Stroke rehabilitation; Virtual reality (VR).
© 2022. The Author(s).
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Lindsay MP, Norrving B, Sacco RL, Brainin M, Hacke W, Martins S, et al. World stroke organization (WSO): global stroke fact sheet 2019. Int J Stroke. 2019;14:806–817. - PubMed
-
- Hendricks HT, Van Limbeek J, Geurts AC, Zwarts MJ. Motor recovery after stroke: a systematic review of the literature. Arch Phys Med Rehabil. 2002;83:1629–1637. - PubMed
-
- Kwakkel G, Kollen BJ, van der Grond J, Prevo AJ. Probability of regaining dexterity in the flaccid upper limb: impact of severity of paresis and time since onset in acute stroke. Stroke. 2003;34:2181–2186. - PubMed
-
- Desrosiers J, Malouin F, Bourbonnais D, Richards CL, Rochette A, Bravo G. Arm and leg impairments and disabilities after stroke rehabilitation: relation to handicap. Clin Rehabil. 2003;17:666–673. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
