

Association between the plasma-to-red blood cell ratio and survival in geriatric and non-geriatric trauma patients undergoing massive transfusion: a retrospective cohort study
- PMID: 35016735
- PMCID: PMC8753889
- DOI: 10.1186/s40560-022-00595-7
Association between the plasma-to-red blood cell ratio and survival in geriatric and non-geriatric trauma patients undergoing massive transfusion: a retrospective cohort study
Abstract
Background: The benefits of a high plasma-to-red blood cell (RBC) ratio on the survival of injured patients who receive massive transfusions remain unclear, especially in older patients. We aimed to investigate the interaction of age with the plasma-to-RBC ratio and clinical outcomes of trauma patients.
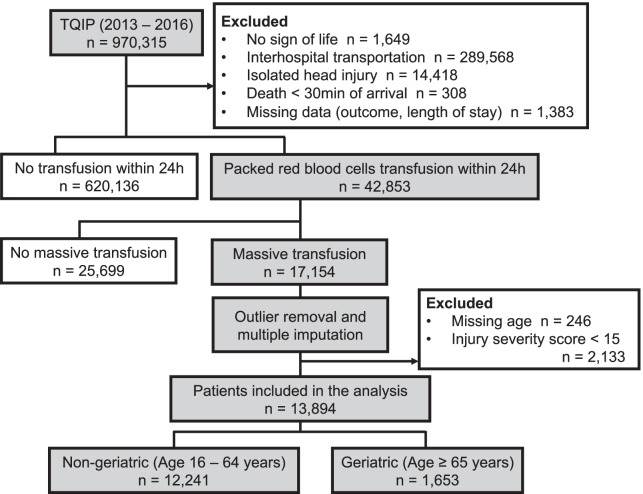
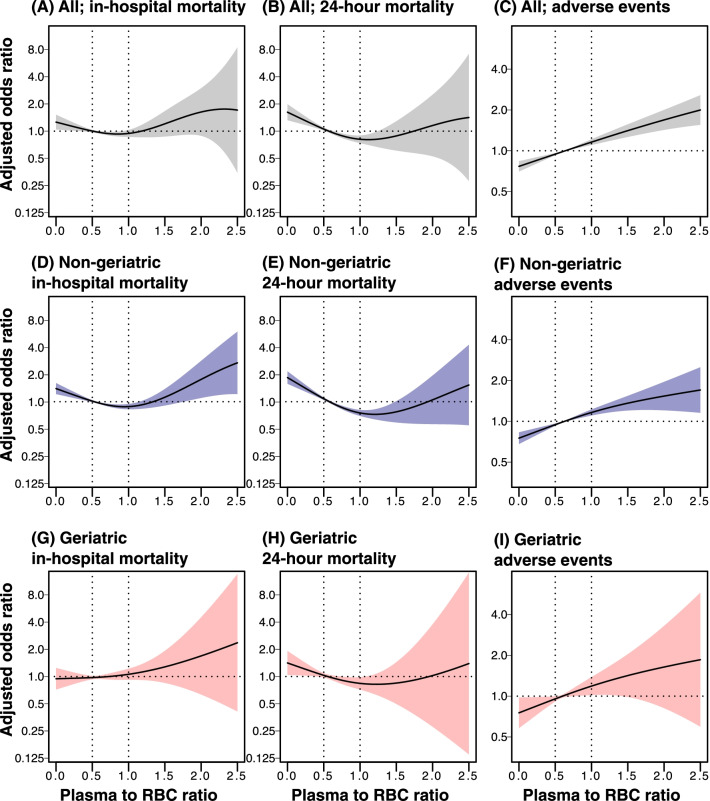
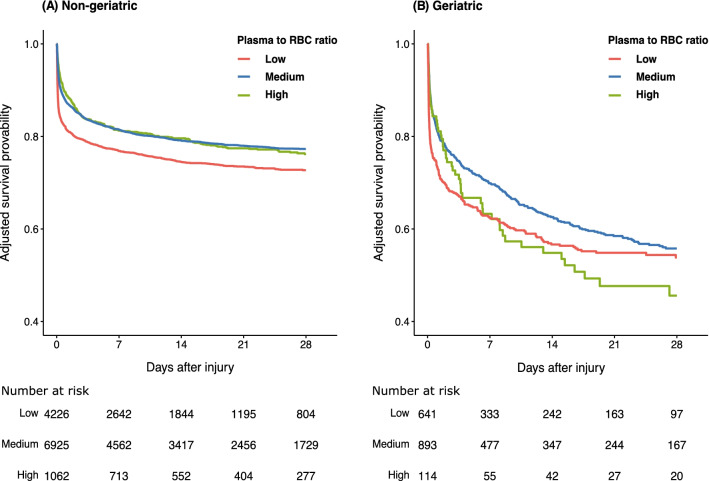
Methods: In this retrospective study conducted from 2013 to 2016, trauma patients who received massive transfusions were included. Using a generalized additive model (GAM),we assessed how the plasma-to-RBC ratio and age affected the in-hospital mortality rates. The association of the plasma-to-RBC ratio [low (< 0.5), medium (0.5-1.0), and high (≥ 1.0)] with in-hospital mortality and the incidence of adverse events were assessed for the overall cohort and for patients stratified into non-geriatric (16-64 years) and geriatric (≥ 65 years) groups using logistic regression analyses.
Results: In total, 13,894 patients were included. The GAM plot of the plasma-to-RBC ratio for in-hospital mortality demonstrated a downward convex unimodal curve for the entire cohort. The low-transfusion ratio group was associated with increased odds of in-hospital mortality in the non-geriatric cohort [odds ratio 1.38, 95% confidence interval (CI) 1.22-1.56]; no association was observed in the geriatric group (odds ratio 0.84, 95% CI 0.62-1.12). An increase in the transfusion ratio was associated with a higher incidence of adverse events in the non-geriatric and geriatric groups.
Conclusion: The association of the non-geriatric age category and plasma-to-RBC ratio for in-hospital mortality was clearly demonstrated. However, the relationship between the plasma-to-RBC ratio with mortality among geriatric patients remains inconclusive.
Keywords: Damage control resuscitation; Geriatric trauma; Massive transfusion; Trauma registry.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that there are no competing financial interests
Figures
References
-
- Cannon JW, Khan MA, Raja AS, Cohen MJ, Como JJ, Cotton BA, et al. Damage control resuscitation in patients with severe traumatic hemorrhage: a practice management guideline from the Eastern Association for the Surgery of Trauma. J Trauma Acute Care Surg. 2017;82:605–617. doi: 10.1097/ta.0000000000001333. - DOI - PubMed
-
- Gonzalez E, Moore EE, Moore HB, Chapman MP, Chin TL, Ghasabyan A, et al. Goal-directed hemostatic resuscitation of trauma-induced coagulopathy: a pragmatic randomized clinical trial comparing a viscoelastic assay to conventional coagulation assays. Ann Surg. 2016;263:1051–1059. doi: 10.1097/sla.0000000000001608. - DOI - PMC - PubMed
-
- Stewart RM, Park PK, Hunt JP, McIntyre RC, Jr., McCarthy J, Zarzabal LA, et al. Less is more: improved outcomes in surgical patients with conservative fluid administration and central venous catheter monitoring. J Am Coll Surg. 2009;208:725–35; discussion 35–7. 10.1016/j.jamcollsurg.2009.01.026. - PubMed
LinkOut - more resources
Full Text Sources
