

Characteristics, contacts, and relative risk of SARS-CoV-2 infection among children during school closures
- PMID: 35016846
- PMCID: PMC8719363
- DOI: 10.1016/j.jmii.2021.12.004
Characteristics, contacts, and relative risk of SARS-CoV-2 infection among children during school closures
Abstract
Background: Characteristics of children with severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) in Taiwanese households is nascent. We sought to characterize SARS-CoV-2 infection, and estimate the relative risk of infection among children within households during school closures in Taipei and New Taipei City.
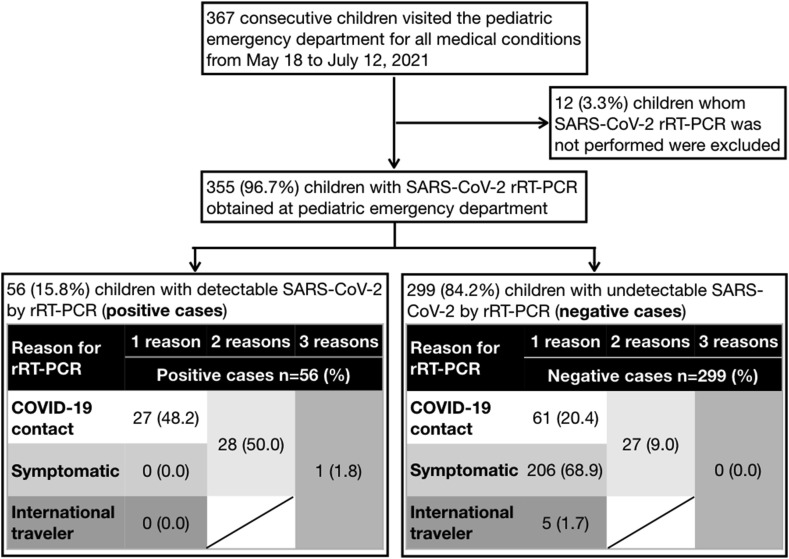
Methods: We reviewed consecutive children below 18 years presenting to our emergency department from May 18, 2021 to July 12, 2021 who underwent real-time reverse-transcription polymerase chain reaction (rRT-PCR) for SARS-CoV-2 from respiratory swabs. Demographics, symptoms, and contacts were captured from medical records. Household contact was defined as an individual with confirmed COVID-19 living in the same residence as the child.
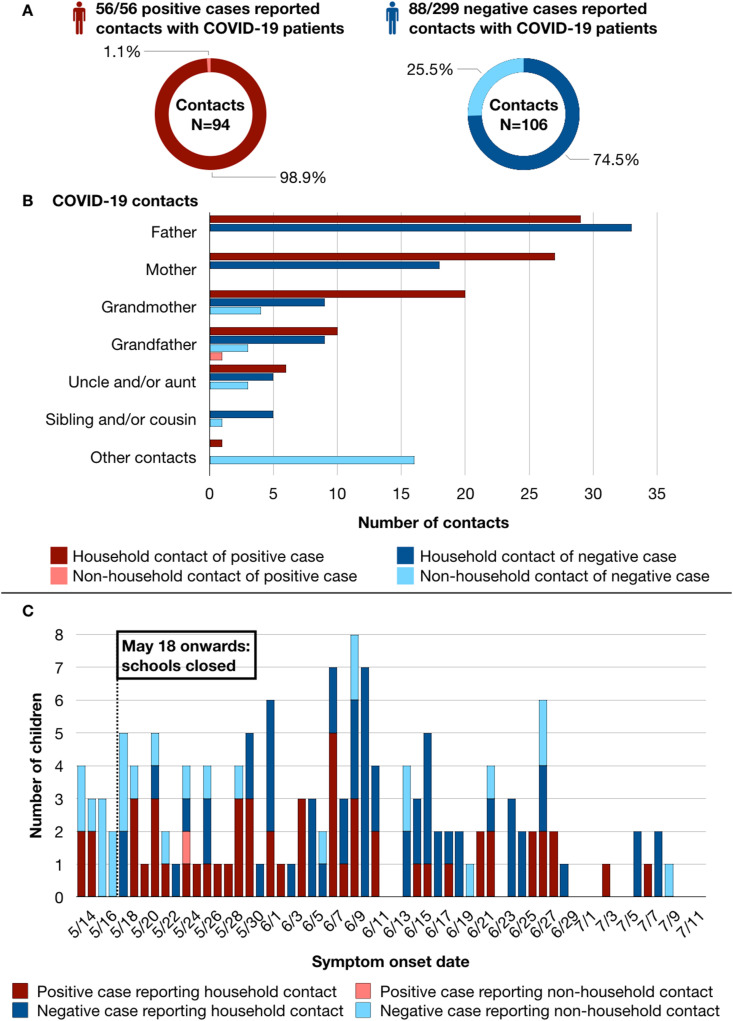
Results: Among 56 children with SARS-CoV-2, twenty-five (45%) were male with mean age of 7.9 years. Symptoms were nonspecific, with 29% having fever, 32% having cough, and 48% were asymptomatic. The median cycle threshold (Ct) value of SARS-CoV-2 rRT-PCR was 25 (range 11-38). All 56 children reported 94 contacts with a COVID-19 patient, of which 99% were household contacts. The relative risk of infection was 8.5 (95% CI 5.0-14.7) for children whose parent(s) were COVID-19 patients, and 7.3 (95% CI 4.9-11.0) for children whose household grandparent(s) were patients, as compared to children without respective contacts. Children without COVID-19 contacts were all tested negative.
Conclusions: During school closures in Taipei and New Taipei City, children with SARS-CoV-2 infection in our cohort had one or more COVID-19 contacts, mostly within their households. While diagnosing pediatric COVID-19 is challenging as children were often asymptomatic, those without contacts were likely uninfected.
Keywords: COVID-19; Children; Household; SARS-CoV-2; School closure; Taiwan.
Copyright © 2022. Published by Elsevier B.V.
Figures
References
-
- Lewis N.M., Chu V.T., Ye D., Conners E.E., Gharpure R., Laws R.L., et al. Household transmission of SARS-CoV-2 in the United States. Clin Infect Dis. 2020 doi: 10.1093/cid/ciaa1166. Epub 2020 Aug 16. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
