

The immune modifying effects of chemotherapy and advances in chemo-immunotherapy
- PMID: 35016920
- PMCID: PMC9271143
- DOI: 10.1016/j.pharmthera.2022.108111
The immune modifying effects of chemotherapy and advances in chemo-immunotherapy
Abstract
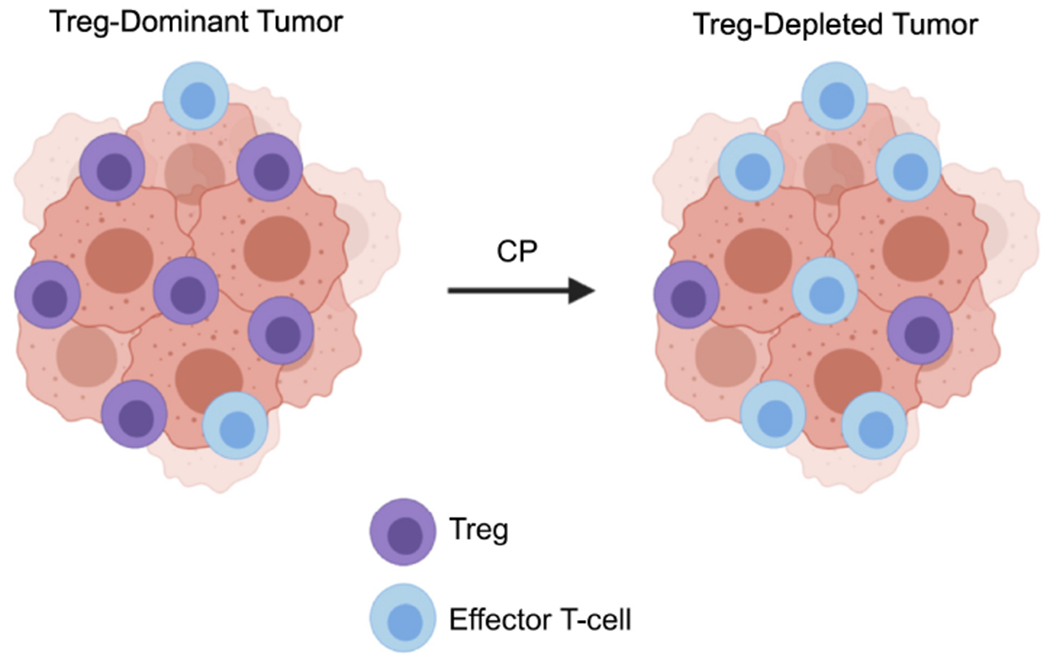
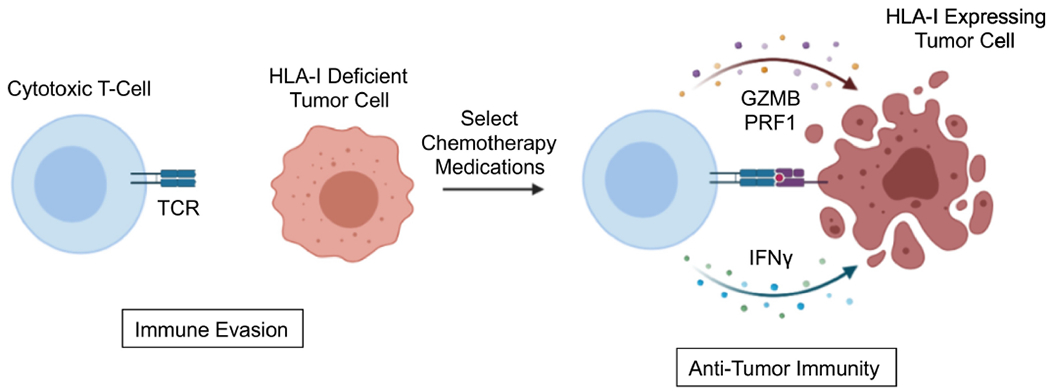
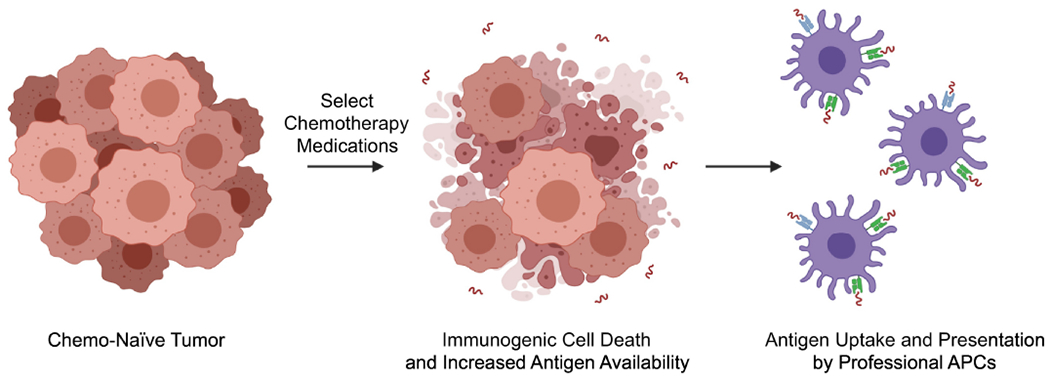
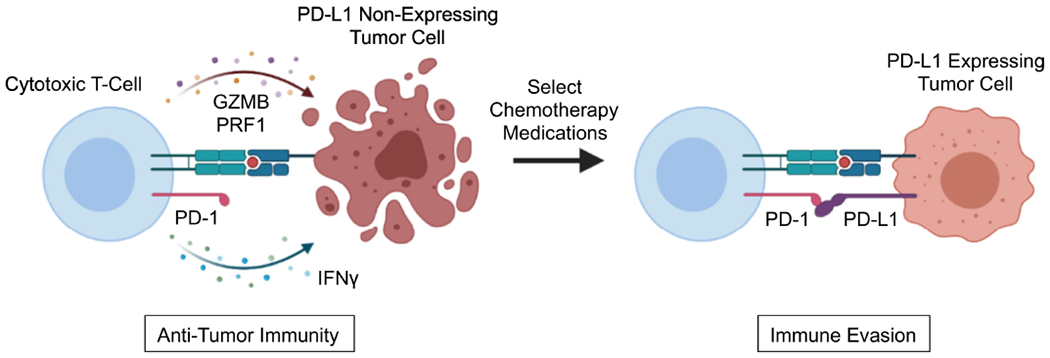
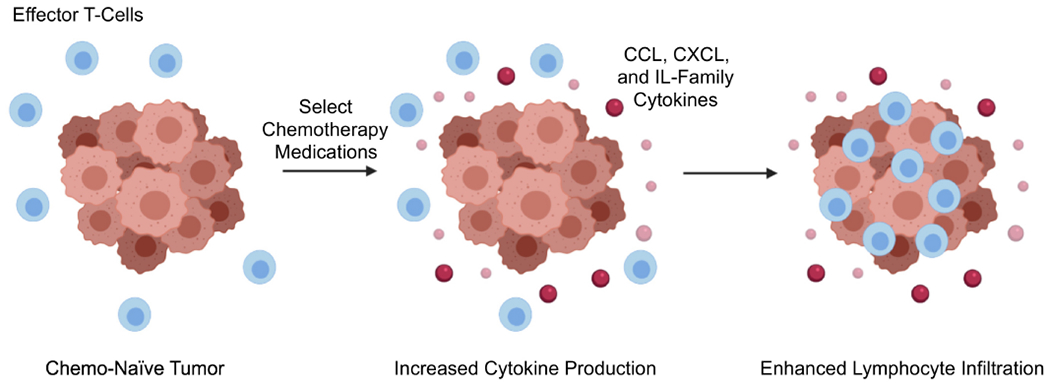
Immune checkpoint inhibitors (ICIs) have transformed the treatment paradigm for several malignancies. While the use of single-agent or combined ICIs has achieved acceptable disease control rates in a variety of solid tumors, such approaches have yet to show substantial therapeutic efficacy in select difficult-to-treat cancer types. Recently, select chemotherapy regimens are emerging as extensive modifiers of the tumor microenvironment, leading to the reprogramming of local immune responses. Accordingly, data is now emerging to suggest that certain anti-neoplastic agents modulate various immune cell processes, most notably the cross-presentation of tumor antigens, leukocyte trafficking, and cytokine biosynthesis. As such, the combination of ICIs and cytotoxic chemotherapy are beginning to show promise in many cancers that have long been considered poorly responsive to ICI-based immunotherapy. Here, we discuss past and present attempts to advance chemo-immunotherapy in these difficult-to-treat cancer histologies, mechanisms through which select chemotherapies modify tumor immunogenicity, as well as important considerations when designing such approaches to maximize efficacy and improve therapeutic response rates.
Keywords: Cancer; Chemotherapy; Immune checkpoint inhibitors; Immunology; Tumor microenvironment.
Copyright © 2022 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors have no conflicts to disclose.
Figures
References
-
- Adams S, Dieras V, Barrios CH, Winer EP, Schneeweiss A, Iwata H, Loi S, Patel S, Henschel V, Chui SY, Rugo HS, Emens LA, & Schmid P (2020). Patient-reported outcomes from the phase III IMpassion130 trial of atezolizumab plus nab-paclitaxel in metastatic triple-negative breast cancer. Ann Oncol, 31, 582–589. - PubMed
-
- Aglietta M, Barone C, Sawyer MB, Moore MJ, Miller WH Jr., Bagala C, Colombi F, Cagnazzo C, Gioeni L, Wang E, Huang B, Fly KD, & Leone F (2014). A phase I dose escalation trial of tremelimumab (CP-675,206) in combination with gemcitabine in chemotherapy-naive patients with metastatic pancreatic cancer. Ann Oncol, 25, 1750–1755. - PubMed
-
- Ahmed AR, & Hombal SM (1984). Cyclophosphamide (Cytoxan). A review on relevant pharmacology and clinical uses. J Am Acad Dermatol, 11, 1115–1126. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
