

The association between vital signs and clinical outcomes in emergency department patients of different age categories
- PMID: 35017189
- PMCID: PMC9691829
- DOI: 10.1136/emermed-2020-210628
The association between vital signs and clinical outcomes in emergency department patients of different age categories
Abstract
Background: Appropriate interpretation of vital signs is essential for risk stratification in the emergency department (ED) but may change with advancing age. In several guidelines, risk scores such as the Systemic Inflammatory Response Syndrome (SIRS) and Quick Sequential Organ Failure Assessment (qSOFA) scores, commonly used in emergency medicine practice (as well as critical care) specify a single cut-off or threshold for each of the commonly measured vital signs. Although a single cut-off may be convenient, it is unknown whether a single cut-off for vital signs truly exists and if the association between vital signs and in-hospital mortality differs per age-category.
Aims: To assess the association between initial vital signs and case-mix adjusted in-hospital mortality in different age categories.
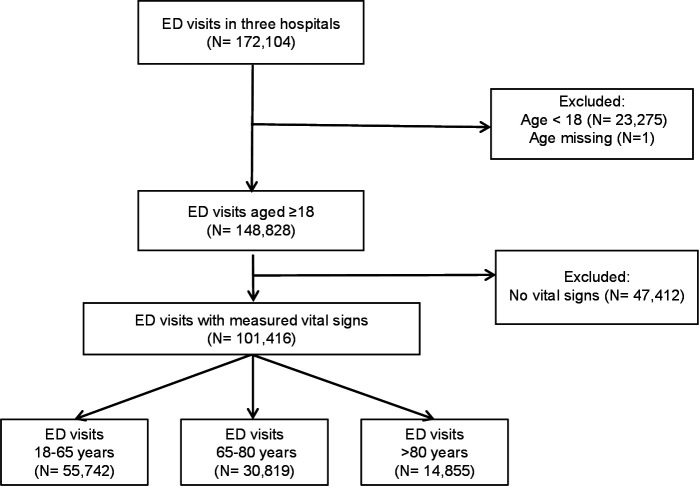
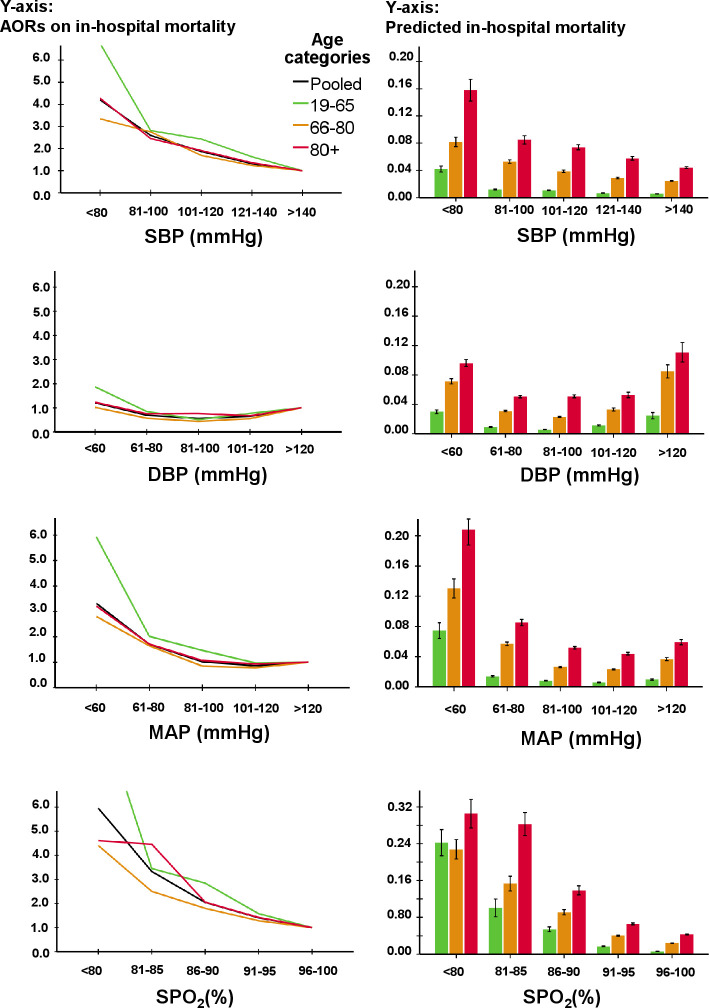
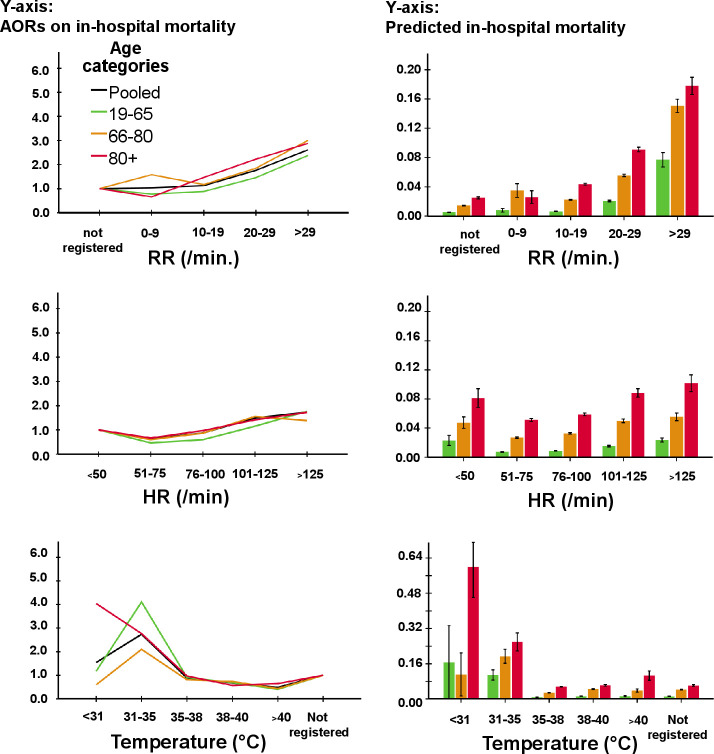
Methods: Observational multicentre cohort study using the Netherlands Emergency Department Evaluation Database (NEED) in which consecutive ED patients ≥18 years were included between 1 January 2017 and 12 January 2020. The association between vital signs and case-mix adjusted mortality were assessed in three age categories (18-65; 66-80; >80 years) using multivariable logistic regression. Vital signs were each divided into five to six categories, for example, systolic blood pressure (SBP) categories (≤80, 81-100, 101-120, 121-140, >140 mm Hg).
Results: We included 101 416 patients of whom 2374 (2.3%) died. Adjusted ORs for mortality increased gradually with decreasing SBP and decreasing peripheral oxygen saturation (SpO2). Diastolic blood pressure (DBP), mean arterial pressure (MAP) and heart rate (HR) had quasi-U-shaped associations with mortality. Mortality did not increase for temperatures anywhere in the range between 35.5°C and 42.0°C, with a single cut-off around 35.5°C below which mortality increased. Single cut-offs were also found for MAP <70 mm Hg and respiratory rate >22/min. For all vital signs, older patients had larger increases in absolute mortality compared with younger patients.
Conclusion: For SBP, DBP, SpO2 and HR, no single cut-off existed. The impact of changing vital sign categories on prognosis was larger in older patients. Our results have implications for the interpretation of vital signs in existing risk stratification tools and acute care guidelines.
Keywords: emergency department; geriatrics; risk management; triage.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
The association between systolic blood pressure and in-hospital mortality in older emergency department patients who are hospitalised with a suspected infection.Emerg Med J. 2018 Oct;35(10):619-622. doi: 10.1136/emermed-2018-207502. Epub 2018 Jul 7. Emerg Med J. 2018. PMID: 29982193
-
The prevalence and diagnostic utility of systemic inflammatory response syndrome vital signs in a pediatric emergency department.Acad Emerg Med. 2015 Apr;22(4):381-9. doi: 10.1111/acem.12610. Epub 2015 Mar 16. Acad Emerg Med. 2015. PMID: 25778743
-
Poor performance of quick-SOFA (qSOFA) score in predicting severe sepsis and mortality - a prospective study of patients admitted with infection to the emergency department.Scand J Trauma Resusc Emerg Med. 2017 Jun 9;25(1):56. doi: 10.1186/s13049-017-0399-4. Scand J Trauma Resusc Emerg Med. 2017. PMID: 28599661 Free PMC article.
-
Head-to-head comparison of qSOFA and SIRS criteria in predicting the mortality of infected patients in the emergency department: a meta-analysis.Scand J Trauma Resusc Emerg Med. 2018 Jul 11;26(1):56. doi: 10.1186/s13049-018-0527-9. Scand J Trauma Resusc Emerg Med. 2018. PMID: 29996880 Free PMC article. Review.
-
Can I Discharge This Adult Patient with Abnormal Vital Signs From the Emergency Department?J Emerg Med. 2024 Nov;67(5):e487-e493. doi: 10.1016/j.jemermed.2024.05.009. Epub 2024 May 19. J Emerg Med. 2024. PMID: 39232943 Review.
Cited by
-
The role of vital signs in predicting mortality risk in elderly patients visiting the emergency department.BMC Emerg Med. 2025 Aug 1;25(1):144. doi: 10.1186/s12873-025-01307-8. BMC Emerg Med. 2025. PMID: 40750848 Free PMC article.
-
The effect of relative hypotension on 30-day mortality in older people receiving emergency care.Intern Emerg Med. 2024 Apr;19(3):787-795. doi: 10.1007/s11739-023-03468-5. Epub 2023 Nov 8. Intern Emerg Med. 2024. PMID: 37940793 Free PMC article.
-
Development and External Validation of the International Early Warning Score for Improved Age- and Sex-Adjusted In-Hospital Mortality Prediction in the Emergency Department.Crit Care Med. 2023 Jul 1;51(7):881-891. doi: 10.1097/CCM.0000000000005842. Epub 2023 Mar 23. Crit Care Med. 2023. PMID: 36951452 Free PMC article.
-
Mortality rates among adult critical care patients with unusual or extreme values of vital signs and other physiological parameters: a retrospective study.Acute Crit Care. 2024 May;39(2):304-311. doi: 10.4266/acc.2023.01361. Epub 2024 May 13. Acute Crit Care. 2024. PMID: 38863361 Free PMC article.
-
Clinical characteristics and prognostic factors of sepsis in patients with malignancy.Sci Rep. 2025 Feb 27;15(1):7078. doi: 10.1038/s41598-025-87457-y. Sci Rep. 2025. PMID: 40016348 Free PMC article.
References
-
- Metlay JP, Waterer GW, Long AC, et al. . Diagnosis and treatment of adults with community-acquired pneumonia. An official clinical practice guideline of the American thoracic Society and infectious diseases Society of America. Am J Respir Crit Care Med 2019;200:e45–67. 10.1164/rccm.201908-1581ST - DOI - PMC - PubMed
-
- American College of S, Committee on T . ATLS : advanced trauma life support for doctors : student course manual. Chicago, IL: American College of Surgeons, 2008.
-
- Adams HP, del Zoppo G, Alberts MJ, et al. . Guidelines for the early management of adults with ischemic stroke: a guideline from the American heart Association/American stroke association stroke Council, clinical cardiology Council, cardiovascular radiology and intervention Council, and the atherosclerotic peripheral vascular disease and quality of care outcomes in research interdisciplinary working groups: the American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Stroke 2007;38:1655–711. 10.1161/STROKEAHA.107.181486 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical