

Effect of a low-salt diet on chronic kidney disease outcomes: a systematic review and meta-analysis
- PMID: 35017237
- PMCID: PMC8753423
- DOI: 10.1136/bmjopen-2021-050843
Effect of a low-salt diet on chronic kidney disease outcomes: a systematic review and meta-analysis
Abstract
Objective: The benefits of a low-salt diet for patients with chronic kidney disease (CKD) are controversial. We conducted a systematic review and meta-analysis of the effect of a low-salt diet on major clinical outcomes.
Design: Systematic review and meta-analysis.
Data sources: MEDLINE by Ovid, EMBASE and the Cochrane Library databases.
Eligibility criteria for selecting studies: We included randomised controlled trials (RCTs) and cohort studies that assessed the effect of a low-salt diet on the renal composite outcomes (more than 50% decline in estimated glomerular filtration rate (eGFR) during follow-up, doubling of serum creatinine or end-stage renal disease), rate of eGFR decline, change in proteinuria, all-cause mortality events, cardiovascular (CV) events, and changes in systolic blood pressure and diastolic blood pressure.
Data extraction and synthesis: Two independent researchers extracted data and evaluated their quality. Relative risks (RRs) with 95% CIs were used for dichotomous data. Differences in means (MDs) or standardised mean differences (SMDs) with 95% CIs were used to pool continuous data. We used the Cochrane Collaboration risk-of-bias tool to evaluate the quality of RCTs, and Newcastle-Ottawa Scale to evaluate the quality of cohort studies.
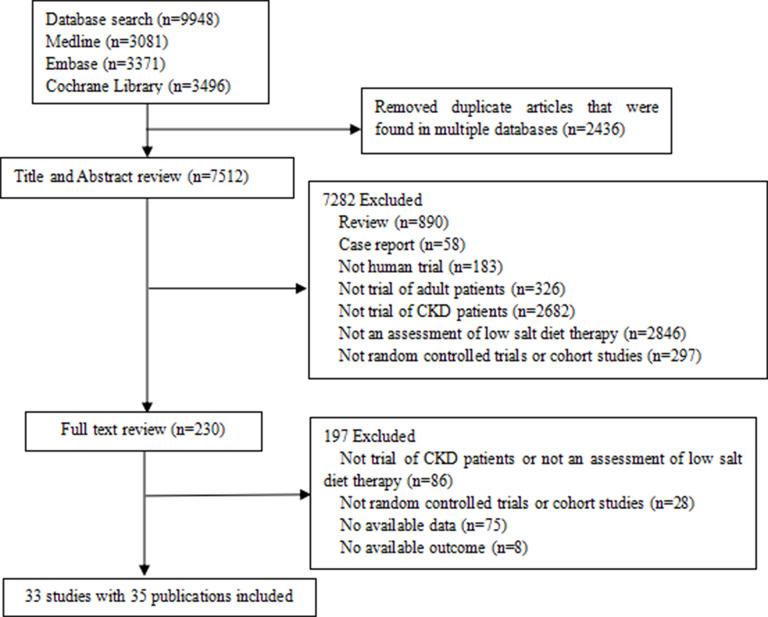
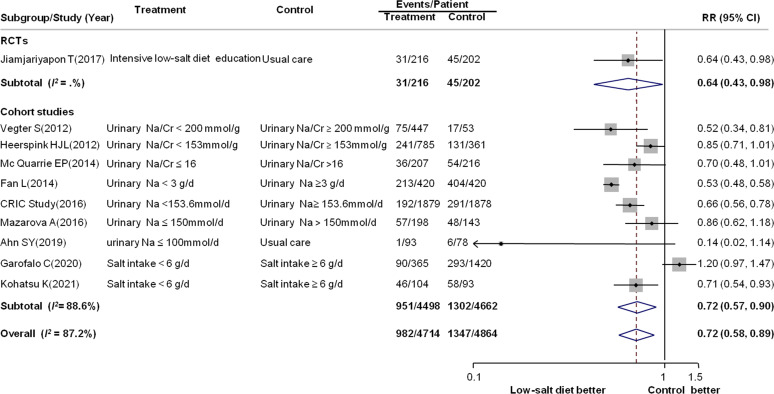
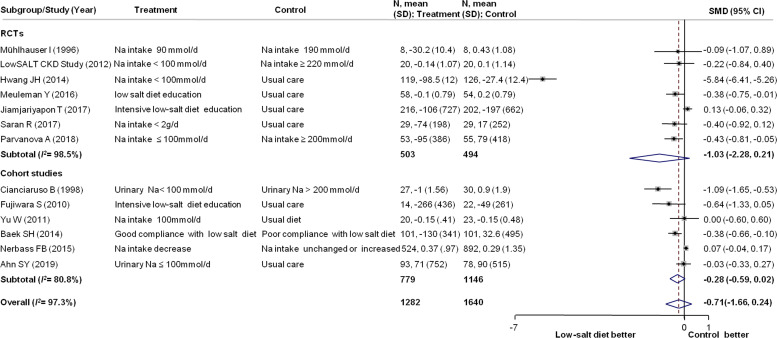
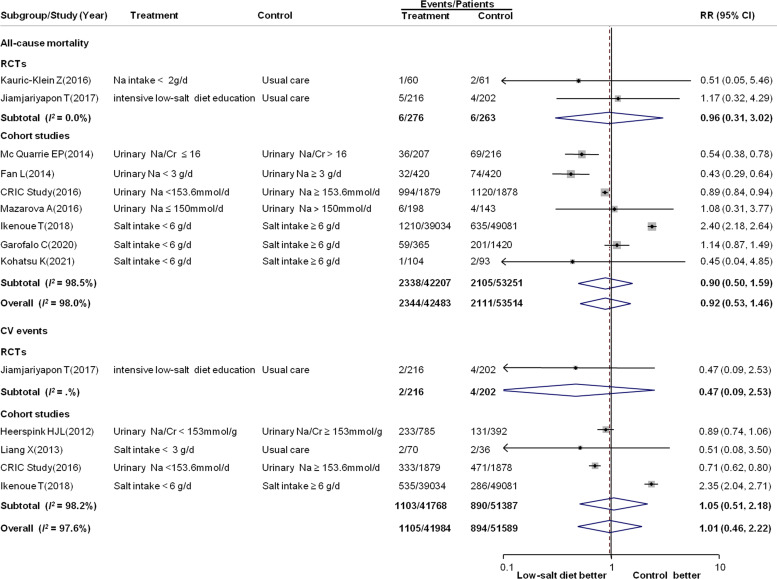
Results: We found 9948 potential research records. After removing duplicates, we reviewed the titles and abstracts, and screened the full text of 230 publications. Thirty-three studies with 101 077 participants were included. A low-salt diet produced a 28% reduction in renal composite outcome events (RR: 0.72; 95% CI: 0.58 to 0.89). No significant effects were found in terms of changes in proteinuria (SMD: -0.71; 95% CI: -1.66 to 0.24), rate of eGFR (decline MD: 1.16; 95% CI: -2.02 to 4.33), risk of all-cause mortality (RR: 0.92; 95% CI: 0.58 to 1.46) and CV events (RR: 1.01; 95% CI: 0.46 to 2.22).
Conclusion: A low-salt diet seems to reduce the risk for renal composite outcome events in patients with CKD. However, no compelling evidence indicated that such a diet would reduce the eGFR decline rate, proteinuria, incidence of all-cause mortality and CV events. Further, more definitive studies are needed.
Prospero registration number: CRD42017072395.
Keywords: chronic renal failure; health services administration & management; nephrology.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous