

Editorial
doi: 10.4103/jpn.JPN_36_20.
Epub 2021 Jul 12.
Transoral Odontoidectomy for Pediatric Craniovertebral Junction Anomaly: Is It Redundant Now?
Affiliations
- PMID: 35018174
- PMCID: PMC8706587
- DOI: 10.4103/jpn.JPN_36_20
Item in Clipboard
Editorial
Transoral Odontoidectomy for Pediatric Craniovertebral Junction Anomaly: Is It Redundant Now?
J Pediatr Neurosci.
2021 Apr-Jun.
No abstract available
Conflict of interest statement
There are no conflicts of interest.
Figures

A 9-year-old child presented to us with progressive spastic quadriparesis (Nurick grade IV) and the CT (A) sagittal image showed AAD with basilar invagination. There was severe canal compromise at foramen magnum and posterior arch of atlas was occipitalized. We did transoral odontoidectomy followed by posterior fixation (O-C1-C2). The postoperative (B) axial and (C) sagittal CT-scan shows ventral decompression and adequate funneling of craniovertebral junction. The child improved in postoperative period and after a follow-up of 3-years, the patient is able to walk without support
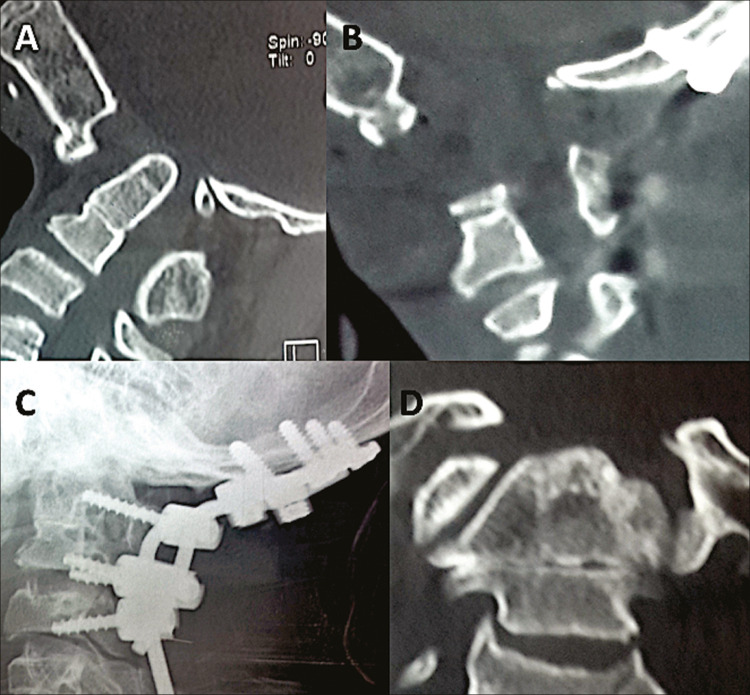
An 11-year-old child presented with acute spastic quadriparesis (Nurick grade III) after a trivial trauma. Radiology showed evidence of atlantoaxial dislocation (A). The patient was operated from posterior approach and occipital-atlas (lateral mass) and axis (pars inter-articularis) fixation was done (C) but the child deteriorated in immediate postoperative period and his ventilator requirement kept on persisting. On the third postoperative day, we did transoral odontoidectomy (B) and patient improved thereafter (D). The child was discharged on the 14th postoperative day and is able to so all his routine activities after 2 years of follow-up

A case of anterior compressive myelopathy due to thick hypertrophied tectorial membrane. (A) Magnetic resonance imaging sagittal T2-weighted sequence of a child operated through posterior fixation and deteriorated (Nurick grade IV, on ventilator). C1–C2 joints were manipulated, reoriented and instrumentation was done. (B, C) After 24 h of the first surgery, excision of hypertrophied tectorial membrane was done and patient improved significantly
References
-
- Sardhara J, Behari S, Sindgikar P, Srivastava AK, Mehrotra A, Das KK, et al. Evaluating atlantoaxial dislocation based on cartesian coordinates: proposing a new definition and its impact on assessment of congenital torticollis. Neurosurgery. 2018;82:525–40. - PubMed
-
- Kanavel AB. Bullet locked between atlas and the base of the skull: technique for removal through the mouth. Surg Clin. 1919;1:361–6.
Publication types
LinkOut - more resources
Full Text Sources