

CVIT expert consensus document on primary percutaneous coronary intervention (PCI) for acute myocardial infarction (AMI) update 2022
- PMID: 35018605
- PMCID: PMC8789715
- DOI: 10.1007/s12928-021-00829-9
CVIT expert consensus document on primary percutaneous coronary intervention (PCI) for acute myocardial infarction (AMI) update 2022
Abstract
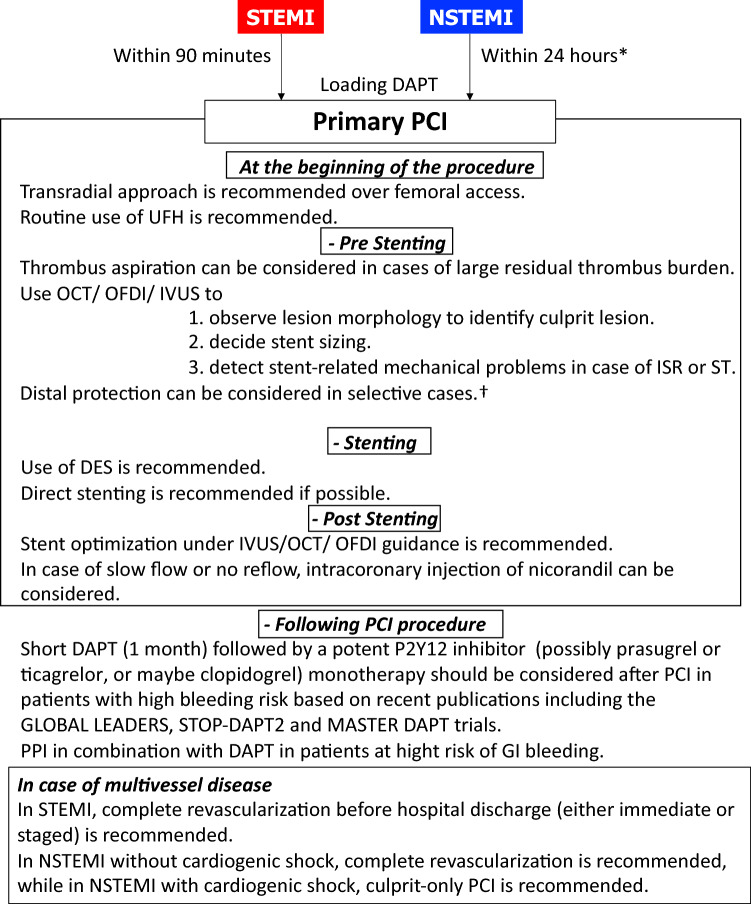
Primary Percutaneous Coronary Intervention (PCI) has significantly contributed to reducing the mortality of patients with ST-segment elevation myocardial infarction (STEMI) even in cardiogenic shock and is now the standard of care in most of Japanese institutions. The Task Force on Primary PCI of the Japanese Association of Cardiovascular Interventional and Therapeutics (CVIT) society proposed an expert consensus document for the management of acute myocardial infarction (AMI) focusing on procedural aspects of primary PCI in 2018. Updated guidelines for the management of AMI were published by the European Society of Cardiology (ESC) in 2017 and 2020. Major changes in the guidelines for STEMI patients included: (1) radial access and drug-eluting stents (DES) over bare-metal stents (BMS) were recommended as a Class I indication, (2) complete revascularization before hospital discharge (either immediate or staged) is now considered as Class IIa recommendation. In 2020, updated guidelines for Non-ST-Elevation Myocardial Infarction (NSTEMI) patients, the followings were changed: (1) an early invasive strategy within 24 h is recommended in patients with NSTEMI as a Class I indication, (2) complete revascularization in NSTEMI patients without cardiogenic shock is considered as Class IIa recommendation, and (3) in patients with atrial fibrillation following a short period of triple antithrombotic therapy, dual antithrombotic therapy (e.g., DOAC and single oral antiplatelet agent preferably clopidogrel) is recommended, with discontinuation of the antiplatelet agent after 6 to 12 months. Furthermore, an aspirin-free strategy after PCI has been investigated in several trials those have started to show the safety and efficacy. The Task Force on Primary PCI of the CVIT group has now proposed the updated expert consensus document for the management of AMI focusing on procedural aspects of primary PCI in 2022 version.
Keywords: Dual antiplatelet therapy (DAPT); Non-ST-segment elevation acute coronary syndrome (NSTE-ACS); Percutaneous coronary intervention (PCI); ST-segment elevation acute myocardial infarction (STEMI); Thrombus aspiration, Optical coherence tomography (OCT).
© 2022. The Author(s).
Figures
References
-
- Hochman JS, Sleeper LA, Webb JG, Sanborn TA, White HD, Talley JD, Buller CE, Jacobs AK, Slater JN, Col J, Mckinlay SM, Lejemtel TH. Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock. N Engl J Med. 1999;341:625–634. doi: 10.1056/nejm199908263410901. - DOI - PubMed
-
- Bonnefoy E, Lapostolle F, Leizorovicz A, Steg G, Mcfadden EP, Dubien PY, Cattan S, Boullenger E, Machecourt J, Lacroute JM, Cassagnes J, Dissait F, Touboul P. Primary angioplasty versus prehospital fibrinolysis in acute myocardial infarction: a randomised study. Lancet (London, England) 2002;360:825–829. doi: 10.1016/s0140-6736(02)09963-4. - DOI - PubMed
-
- Widimsky P, Budesinsky T, Vorac D, Groch L, Zelizko M, Aschermann M, Branny M, St'asek J, Formanek P. Long distance transport for primary angioplasty vs immediate thrombolysis in acute myocardial infarction. Final results of the randomized national multicentre trial–PRAGUE-2. Eur Heart J. 2003;24:94–104. doi: 10.1016/S0195-668X(02)00468-2. - DOI - PubMed
-
- Steg PG, Bonnefoy E, Chabaud S, Lapostolle F, Dubien PY, Cristofini P, Leizorovicz A, Touboul P. Impact of time to treatment on mortality after prehospital fibrinolysis or primary angioplasty: data from the CAPTIM randomized clinical trial. Circulation. 2003;108:2851–2856. doi: 10.1161/01.cir.0000103122.10021.f2. - DOI - PubMed
-
- Lincoff AM, Califf RM, Van De Werf F, Willerson JT, White HD, Armstrong PW, Guetta V, Gibler WB, Hochman JS, Bode C, Vahanian A, Steg PG, Ardissino D, Savonitto S, Bar F, Sadowski Z, Betriu A, Booth JE, Wolski K, Waller M, Topol EJ. Mortality at 1 year with combination platelet glycoprotein IIb/IIIa inhibition and reduced-dose fibrinolytic therapy vs conventional fibrinolytic therapy for acute myocardial infarction: GUSTO V randomized trial. JAMA. 2002;288:2130–2135. doi: 10.1001/jama.288.17.2130. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
