

Vitamins A, D, E status as related to supplementation and lung disease markers in young children with cystic fibrosis
- PMID: 35018747
- PMCID: PMC8930603
- DOI: 10.1002/ppul.25825
Vitamins A, D, E status as related to supplementation and lung disease markers in young children with cystic fibrosis
Abstract
Background: The variable response to fat-soluble vitamin supplementation in young children with cystic fibrosis (CF), and factors contributing to this variability, remain under-investigated.
Objective: To determine if recommended supplement doses normalize serum vitamins A (retinol), D (25-hydroxy-vitamin D, 25OHD), and E (α-tocopherol), and identify factors predictive of achieving sufficiency, in children with CF in the first 3 years of life.
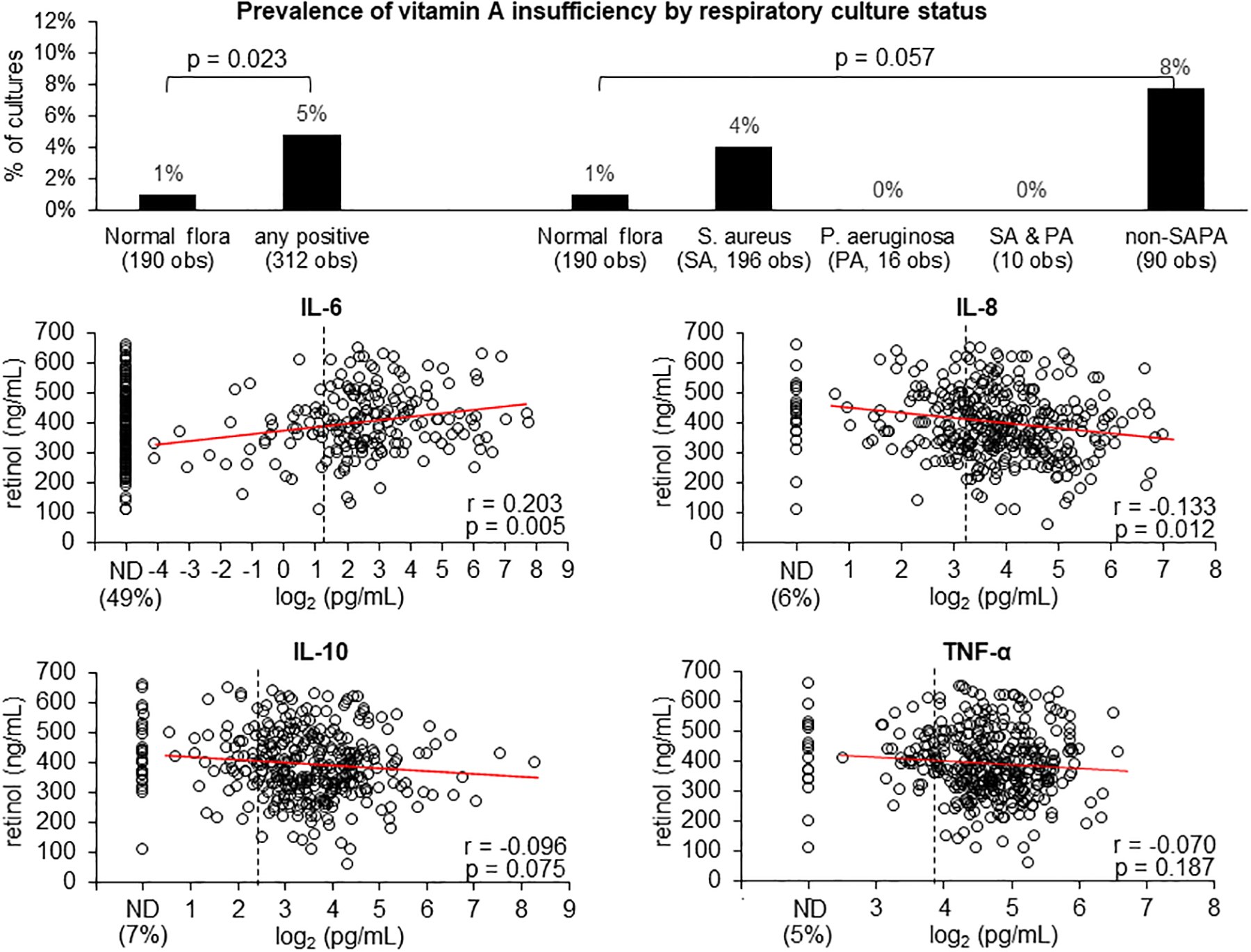
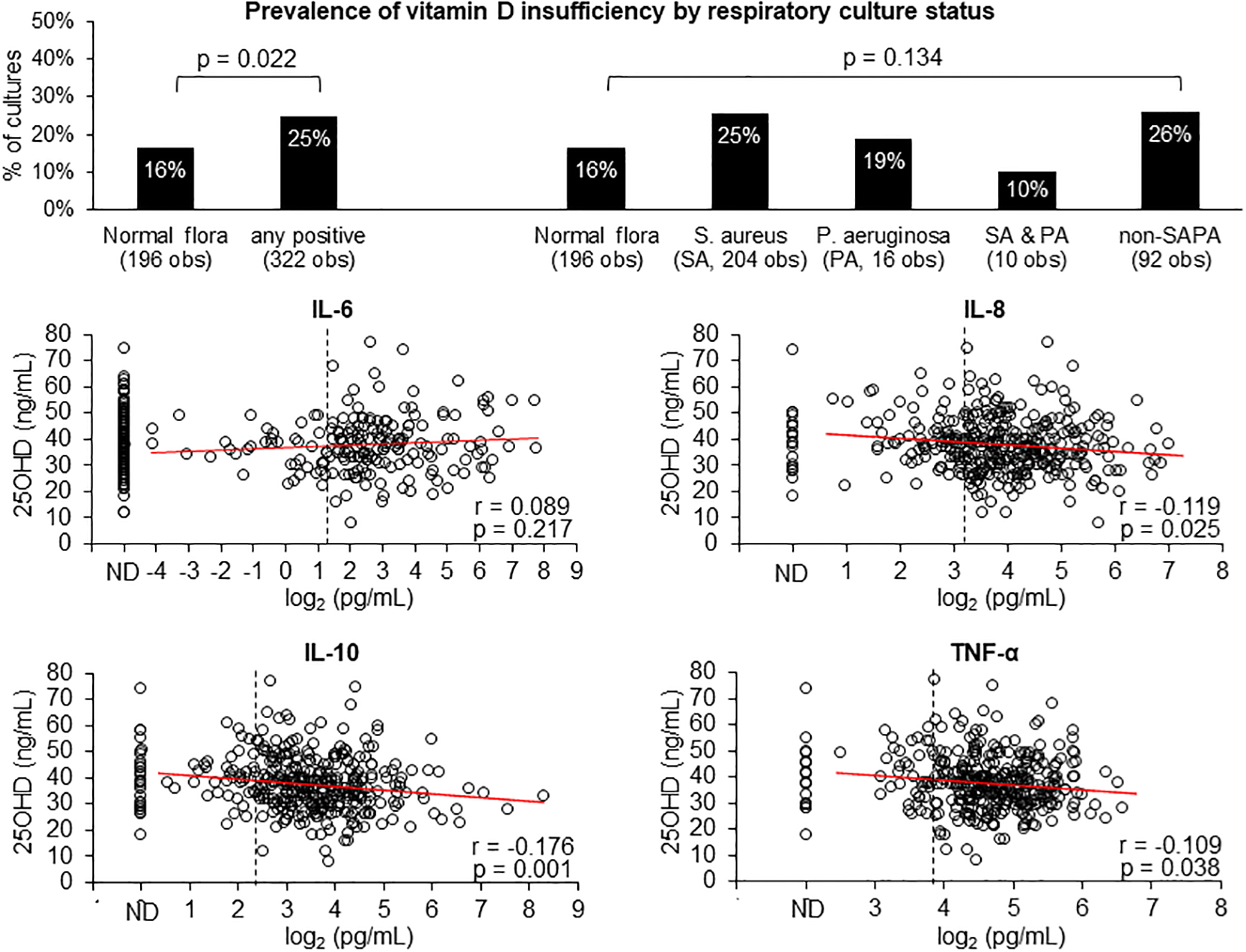
Design: We studied 144 infants born during 2012-2017 and diagnosed with CF through newborn screening. Serum retinol, 25OHD, α-tocopherol and plasma cytokines interleukin (IL)-6, IL-8, IL-10, and tumor necrosis factor (TNF)-α were measured in early infancy and yearly thereafter. Vitamin supplement intakes and respiratory microbiology were assessed every 1-2 months in infancy and quarterly thereafter.
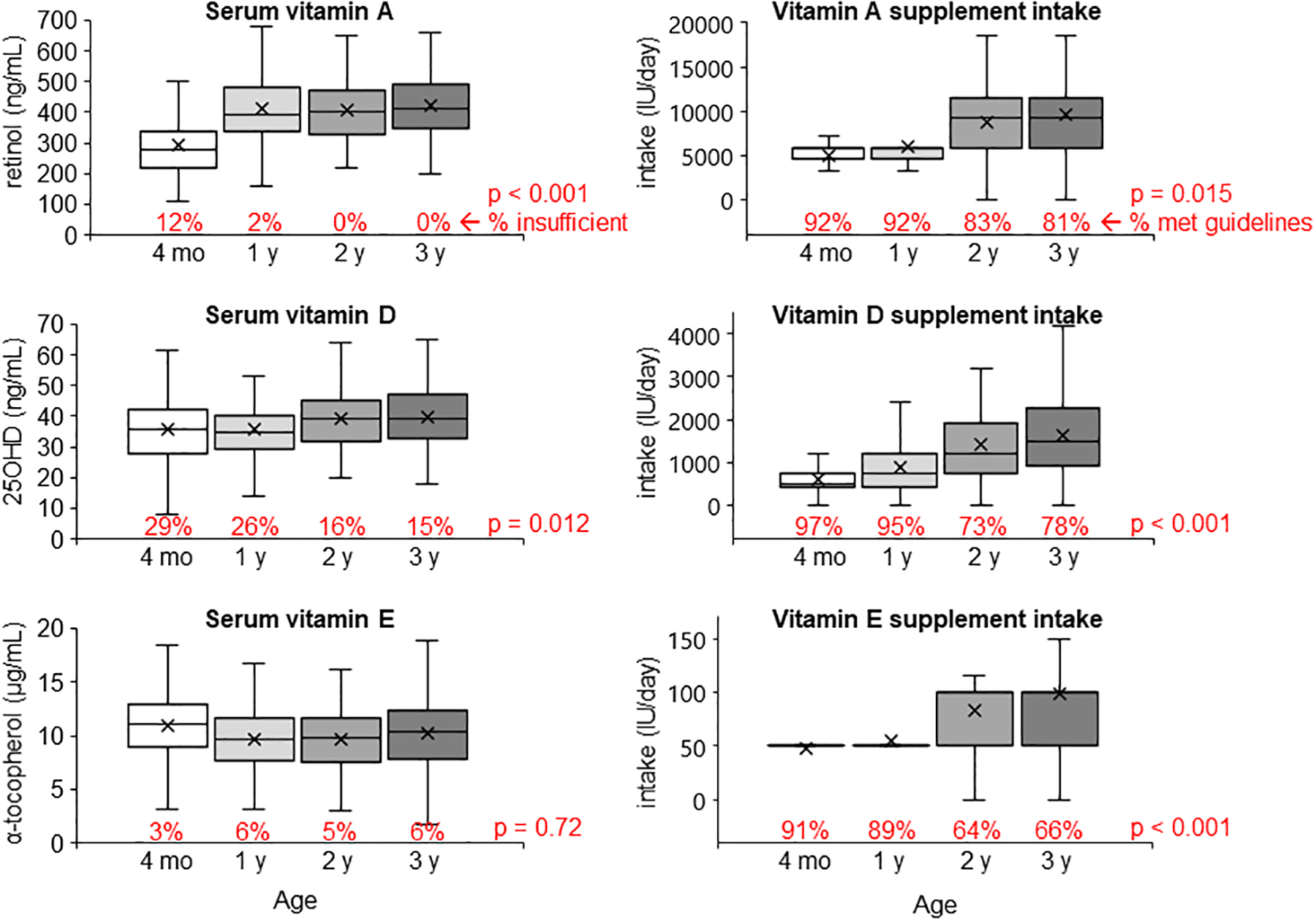
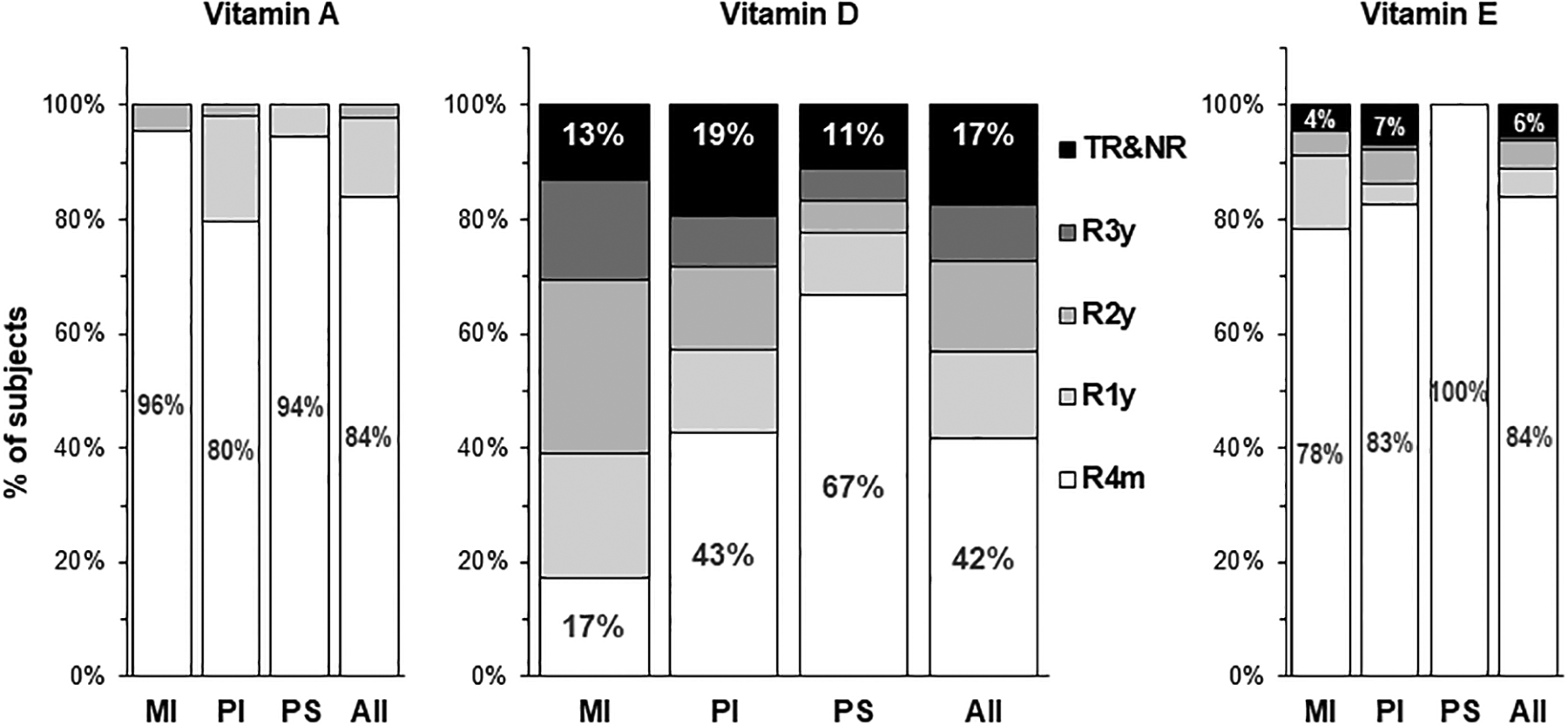
Results: The prevalence of vitamin D insufficiency (<30 ng/ml) at all ages combined was significantly higher (22%) compared to vitamin A (<200 ng/ml, 3%) and vitamin E (<5 µg/ml, 5%). All children were vitamin A sufficient by age 2 years. Vitamin E insufficiency was rare. Only 42% were early responders of vitamin D and 17% remain insufficient despite high supplement intakes. IL-6 was positively correlated, while IL-8, IL-10, and TNF-α were negatively correlated, with retinol and 25OHD. Multiple regression analysis revealed that supplement dose, season, α-tocopherol, pancreatic insufficiency, respiratory infections and IL-10 were significant predictors of 25OHD.
Conclusion: Diagnosis through newborn screening coupled with supplementation normalized serum retinol and α-tocopherol in almost all infants with CF by age 3 years. However, response to vitamin D supplements in young children with CF occurred later and variably despite early and sustained supplementation.
Keywords: 25-hydroxyvitamin D; children; cystic fibrosis; fat-soluble vitamins; infection; inflammation; vitamin A; vitamin D; vitamin D supplementation; vitamin E.
© 2022 Wiley Periodicals LLC.
Conflict of interest statement
Figures
References
-
- Marcus MS, Sondel SA, Farrell PM, Laxova A, Carey PM, Langhough R, Mischler EH. Nutritional status of infants with cystic fibrosis associated with early diagnosis and intervention. Am J Clin Nutr. 1991;54(3):578–585. - PubMed
-
- Bronstein MN, Sokol RJ, Abman SH, Chatfield BA, Hammond KB, Hambidge KM, Stall CD, Accurso FJ. Pancreatic insufficiency, growth, and nutrition in infants identified by newborn screening as having cystic fibrosis. J Pediatr. 1992;120(4):533–540. - PubMed
-
- Wilfond BS, Farrell PM, Laxova A, Mischler E. Severe hemolytic anemia associated with vitamin E deficiency in infants with cystic fibrosis. Implications for neonatal screening. Clin Pediatr (Phila). 1994;33(1):2–7. - PubMed
-
- Borowitz D, Baker RD, Stallings V. Consensus report on nutrition for pediatric patients with cystic fibrosis. J Pediatr Gastroenterol Nutr. 2002;35(3):246–259. - PubMed
-
- Stallings VA, Stark LJ, Robinson KA, Feranchak AP, Quinton H; Clinical Practice Guidelines on Growth and Nutrition Subcommittee; Ad Hoc Working Group. Evidence-based practice recommendations for nutrition-related management of children and adults with cystic fibrosis and pancreatic insufficiency: results of a systematic review. J Am Diet Assoc. 2008;108(5):832–839. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
