

Effects of SGLT2 inhibitors on cardiovascular outcomes in patients with stage 3/4 CKD: A meta-analysis
- PMID: 35020750
- PMCID: PMC8754287
- DOI: 10.1371/journal.pone.0261986
Effects of SGLT2 inhibitors on cardiovascular outcomes in patients with stage 3/4 CKD: A meta-analysis
Abstract
Introduction: After stage 3 CKD, the risk of adverse cardiovascular events increased significantly. Therefore, we performed a meta-analysis to investigate the cardiovascular protective effect of SGLT2 inhibitors in patients with stage 3/4 CKD with different baseline kidney function or underlying diseases.
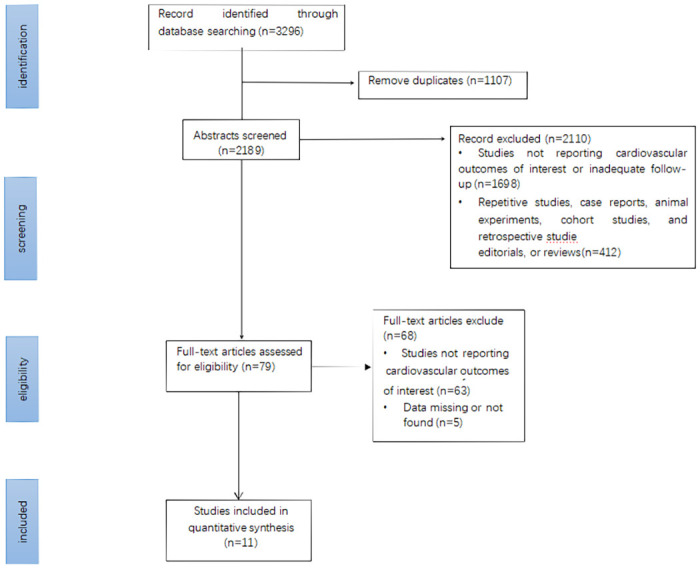
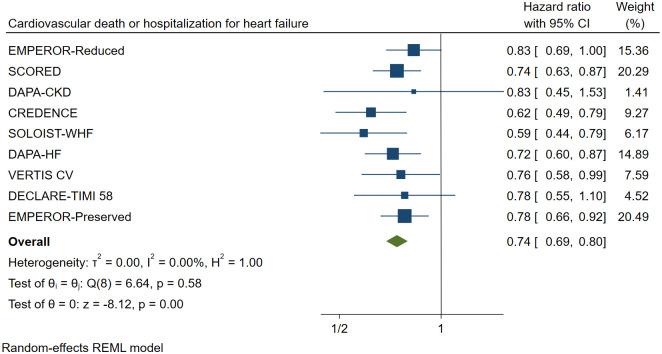
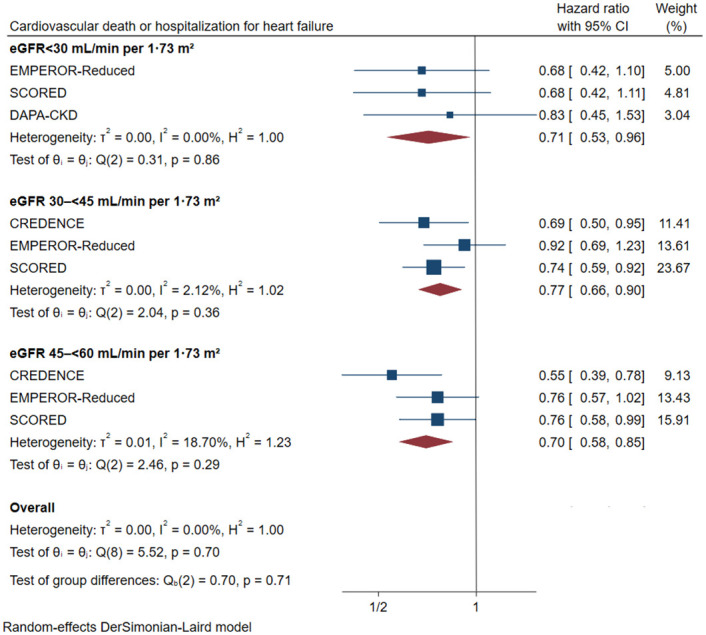
Method: To identify eligible trials, we systematically searched the Embase, PubMed, Web of Science, and Cochrane library databases from inception to April 15, 2021. The primary cardiovascular outcome was defined as a combination of cardiovascular mortality and hospitalization due to heart failure. Baseline kidney functions (stage 3a CKD: eGFR45-59mL/min per 1.73m2, stage 3b CKD: eGFR30-44mL/min per 1.73m2, stage 4 CKD: eGFR<30mL/min per 1.73m2) and underlying diseases (Type 2 diabetes, heart failure (Preserved ejection fraction or reduced ejection fraction), atherosclerotic cardiovascular disease) were used to stratify efficacy and safety outcomes. The results were subjected to a sensitivity analysis to ensure that they were reliable.
Results: In the present study, a total of eleven trials were included that involved a total of 27,823 patients with stage 3/4 CKD. The treatment and control groups contained 14,451 and 13,372 patients, respectively. In individuals with stage 3/4 CKD, SGLT2 inhibitors reduced the risk of primary cardiovascular outcomes by 26% (HR 0.74, [95% CI 0.69-0.80], I2 = 0.00%), by 30% in patients with stage 3a CKD (HR 0.70, [95% CI 0.59-0.84], I2 = 18.70%), by 23% in patients with stage 3b CKD (HR 0.77, [95% CI 0.66-0.90], I2 = 2.12%), and by 29% in patients with stage 4 CKD (HR 0.71, [95% CI 0.53-0.96], I2 = 0.00%). The risk of primary outcomes was reduced by 29% (HR 0.71, [95% CI 0.63-0.80], I2 = 0.00%) in patients with type 2 diabetes, by 28% (HR 0.72, [95% CI 0.56-0.93], I2 = 37.23%) in patients with heart failure with preserved ejection fraction, by 21% (HR 0.79, [95% CI 0.70-0.89], I2 = 0.00%) in patients with heart failure with reduced ejection fraction, and by 25% (HR 0.75, [95% CI 0.64-0.88], I2 = 0.00%) in patients with atherosclerotic cardiovascular disease.
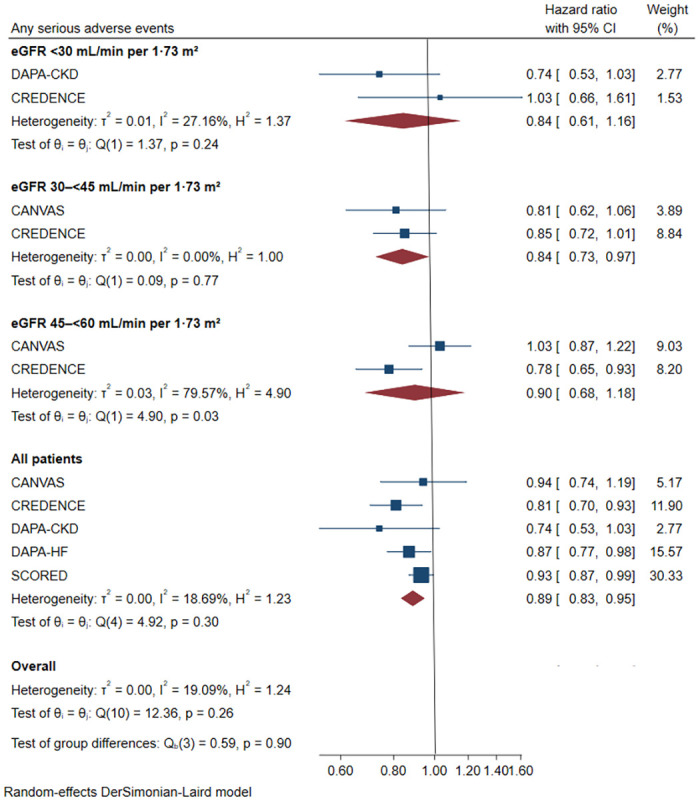
Conclusions: For stage 3/4 CKD, SGLT2 inhibitors significantly decreased the risk of primary cardiovascular outcomes, and these benefits were consistent throughout the spectrum of different kidney functions, even in stage 4 CKD. There was no evidence of increased adverse outcomes across different baseline clinical complications, such as type 2 diabetes, heart failure, or atherosclerotic cardiovascular disease.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
