

Racemic Ketamine as an Alternative to Electroconvulsive Therapy for Unipolar Depression: A Randomized, Open-Label, Non-Inferiority Trial (KetECT)
- PMID: 35020871
- PMCID: PMC9154276
- DOI: 10.1093/ijnp/pyab088
Racemic Ketamine as an Alternative to Electroconvulsive Therapy for Unipolar Depression: A Randomized, Open-Label, Non-Inferiority Trial (KetECT)
Abstract
Background: Ketamine has emerged as a fast-acting and powerful antidepressant, but no head to head trial has been performed, Here, ketamine is compared with electroconvulsive therapy (ECT), the most effective therapy for depression.
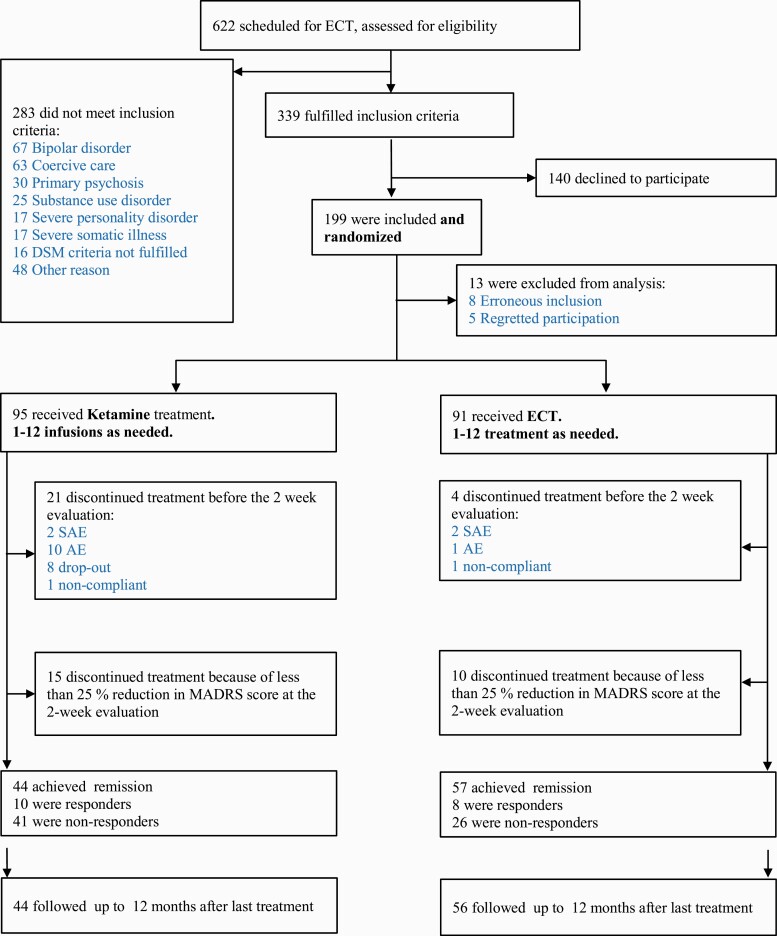
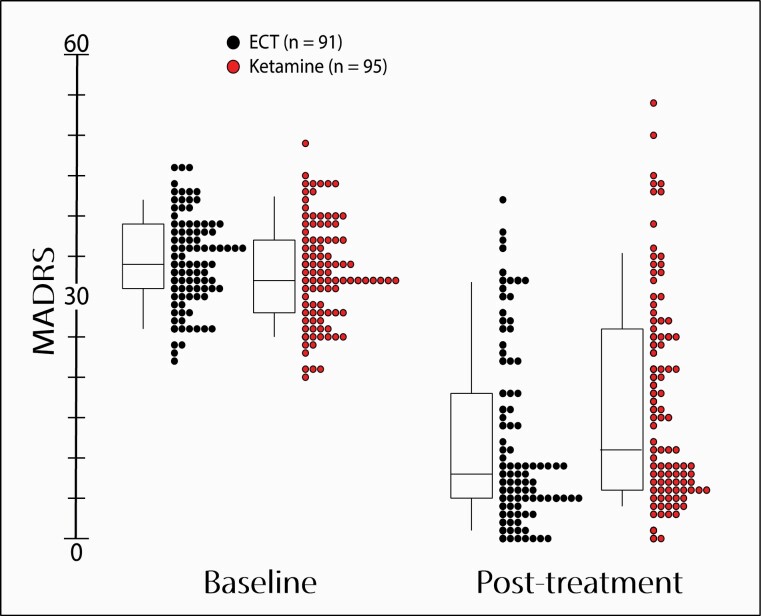
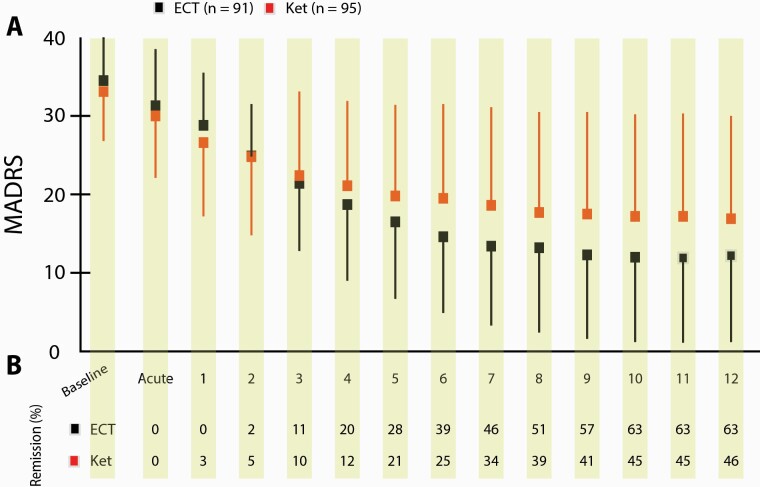
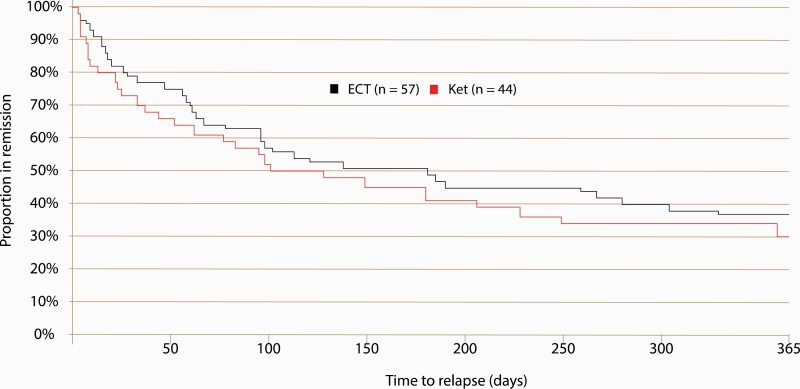
Methods: Hospitalized patients with unipolar depression were randomized (1:1) to thrice-weekly racemic ketamine (0.5 mg/kg) infusions or ECT in a parallel, open-label, non-inferiority study. The primary outcome was remission (Montgomery Åsberg Depression Rating Scale score ≤10). Secondary outcomes included adverse events (AEs), time to remission, and relapse. Treatment sessions (maximum of 12) were administered until remission or maximal effect was achieved. Remitters were followed for 12 months after the final treatment session.
Results: In total 186 inpatients were included and received treatment. Among patients receiving ECT, 63% remitted compared with 46% receiving ketamine infusions (P = .026; difference 95% CI 2%, 30%). Both ketamine and ECT required a median of 6 treatment sessions to induce remission. Distinct AEs were associated with each treatment. Serious and long-lasting AEs, including cases of persisting amnesia, were more common with ECT, while treatment-emergent AEs led to more dropouts in the ketamine group. Among remitters, 70% and 63%, with 57 and 61 median days in remission, relapsed within 12 months in the ketamine and ECT groups, respectively (P = .52).
Conclusion: Remission and cumulative symptom reduction following multiple racemic ketamine infusions in severely ill patients (age 18-85 years) in an authentic clinical setting suggest that ketamine, despite being inferior to ECT, can be a safe and valuable tool in treating unipolar depression.
Keywords: Electroconvulsive therapy; ketamine infusion; major depressive disorder; psychotic depression; racemic ketamine.
© The Author(s) 2021. Published by Oxford University Press on behalf of CINP.
Figures
References
-
- aan het Rot M, Collins KA, Murrough JW, Perez AM, Reich DL, Charney DS, Mathew SJ (2010) Safety and efficacy of repeated-dose intravenous ketamine for treatment-resistant depression. Biol Psychiatry 67:139–145. - PubMed
-
- Berman RM, Cappiello A, Anand A, Oren DA, Heninger GR, Charney DS, Krystal JH (2000) Antidepressant effects of ketamine in depressed patients. Biol Psychiatry 47:351–354. - PubMed
-
- Bremner JD, Krystal JH, Putnam FW, Southwick SM, Marmar C, Charney DS, Mazure CM (1998) Measurement of dissociative states with the Clinician-Administered Dissociative States Scale (CADSS). J Trauma Stress 11:125–136. - PubMed
-
- Caddy C, Amit BH, McCloud TL, Rendell JM, Furukawa TA, McShane R, Hawton K, Cipriani A (2015) Ketamine and other glutamate receptor modulators for depression in adults. Cochrane Database Syst Rev 9:CD011612. - PubMed
-
- Cusin C, Ionescu DF, Pavone KJ, Akeju O, Cassano P, Taylor N, Eikermann M, Durham K, Swee MB, Chang T, Dording C, Soskin D, Kelley J, Mischoulon D, Brown EN, Fava M (2017) Ketamine augmentation for outpatients with treatment-resistant depression: preliminary evidence for two-step intravenous dose escalation. Aust N Z J Psychiatry 51:55–64. - PubMed
