

Optimizing care coordination to address social determinants of health needs for dual-use veterans
- PMID: 35022053
- PMCID: PMC8754195
- DOI: 10.1186/s12913-021-07408-x
Optimizing care coordination to address social determinants of health needs for dual-use veterans
Abstract
Background: Veterans increasingly utilize both the Veteran's Health Administration (VA) and non-VA hospitals (dual-users). Dual-users are at increased risk of fragmented care and adverse outcomes and often do not receive necessary follow-up care addressing social determinants of health (SDOH). We developed a Veteran-informed social worker-led Advanced Care Coordination (ACC) program to decrease fragmented care and provide longitudinal care coordination addressing SDOH for dual-users accessing non-VA emergency departments (EDs) in two communities.
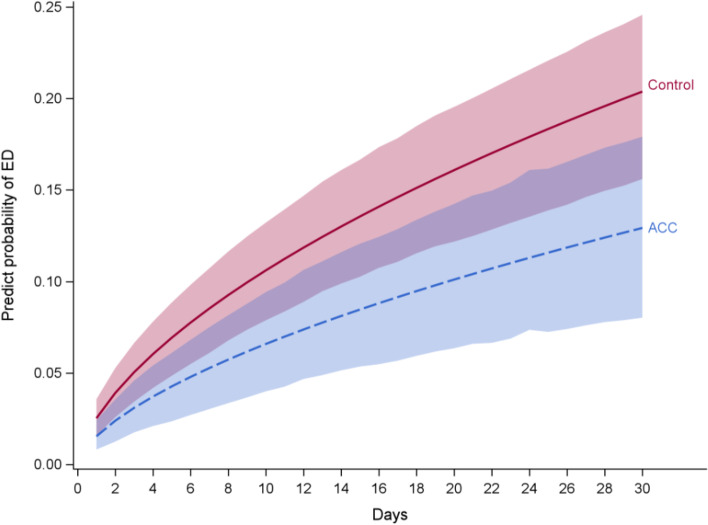
Methods: ACC had four core components: 1. Notification from non-VA ED providers of Veterans' ED visit; 2. ACC social worker completed a comprehensive assessment with the Veteran to identify SDOH needs; 3. Clinical intervention addressing SDOH up to 90 days post-ED discharge; and 4. Warm hand-off to Veteran's VA primary care team. Data was documented in our program database. We performed propensity matching between a control group and ACC participants between 4/10/2018 - 4/1/2020 (N- = 161). A joint survival model using Markov Chain Monte Carlo technique was employed for 30-day outcomes. We performed Difference-In-Difference analyses on number of ED visits, admissions, and primary care physician (PCP) visits 120-day pre/post discharge.
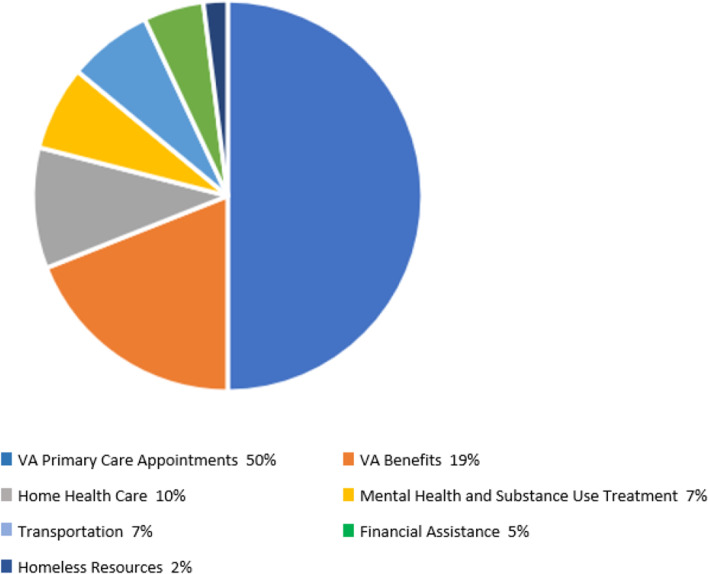
Results: When compared to a matched control group ACC had significantly lower risk of 30-day ED visits (Hazard Ratio (HR) = 0.61, 95% Confidence Interval (CI) = (0.42, 0.92)) and a higher probability of PCP visits at 13-30 days post-ED visit (HR = 1.5, 95% CI = (1.01, 2.22)). Veterans enrolled in ACC were connected to VA PCP visits (50%), VA benefits (19%), home health care (10%), mental health and substance use treatment (7%), transportation (7%), financial assistance (5%), and homeless resources (2%).
Conclusion: We developed and implemented a program addressing dual-users' SDOH needs post non-VA ED discharge. Social workers connected dual-users to needed follow-up care and resources which reduced fragmentation and adverse outcomes.
Keywords: emergency departments; social determinants of health; social work; veterans; veterans health administration.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Tsilimingras D, Bates DW. Addressing post discharge adverse events: a neglected area. Jt Comm J Qual Patient Saf. 2008;34(2):85–97. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
