

Practical guide to cardiopulmonary exercise testing in adults
- PMID: 35022059
- PMCID: PMC8754079
- DOI: 10.1186/s12931-021-01895-6
Practical guide to cardiopulmonary exercise testing in adults
Abstract
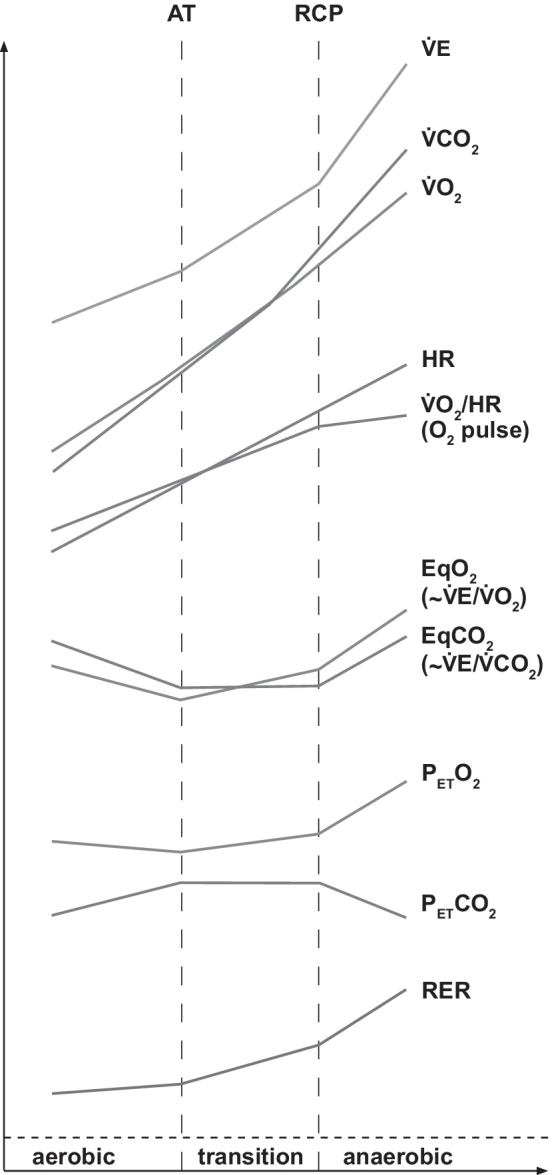
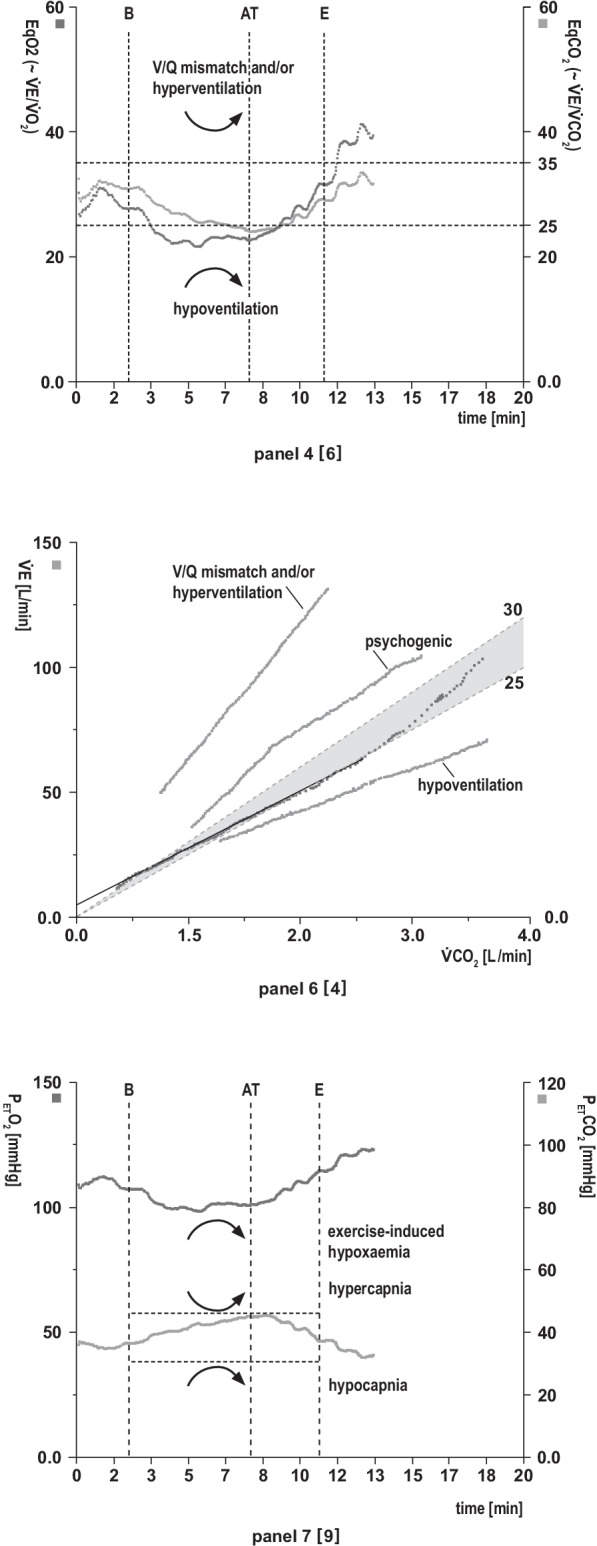
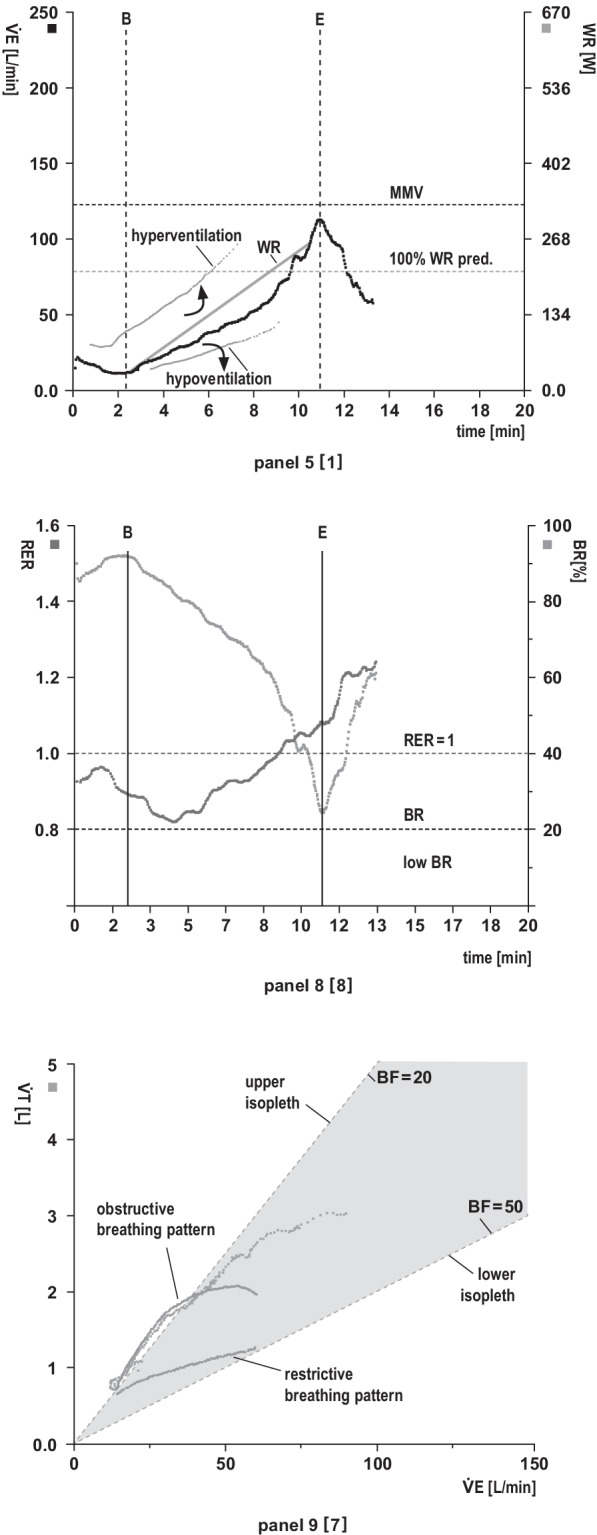
Unexplained exertional dyspnoea or fatigue can arise from a number of underlying disorders and shows only a weak correlation with resting functional or imaging tests. Noninvasive cardiopulmonary exercise testing (CPET) offers a unique, but still under-utilised and unrecognised, opportunity to study cardiopulmonary and metabolic changes simultaneously. CPET can distinguish between a normal and an abnormal exercise response and usually identifies which of multiple pathophysiological conditions alone or in combination is the leading cause of exercise intolerance. Therefore, it improves diagnostic accuracy and patient health care by directing more targeted diagnostics and facilitating treatment decisions. Consequently, CPET should be one of the early tests used to assess exercise intolerance. However, this test requires specific knowledge and there is still a major information gap for those physicians primarily interested in learning how to systematically analyse and interpret CPET findings. This article describes the underlying principles of exercise physiology and provides a practical guide to performing CPET and interpreting the results in adults.
Keywords: 9-Panel plot; COPD; Cardiovascular disease; Dyspnea; Exercise limitation; Interstitial lung disease; Pulmonary hypertension; Ventilatory inefficiency.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Sietsema KE, Sue DY, Stringer WW, Ward SA. Wasserman & Whipp’s principles of exercise testing and interpretation. 6. Philadelphia: Wolters Kluwer; 2021.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
