

Innate immune deficiencies are associated with severity and poor prognosis in patients with COVID-19
- PMID: 35022495
- PMCID: PMC8755788
- DOI: 10.1038/s41598-021-04705-7
Innate immune deficiencies are associated with severity and poor prognosis in patients with COVID-19
Abstract
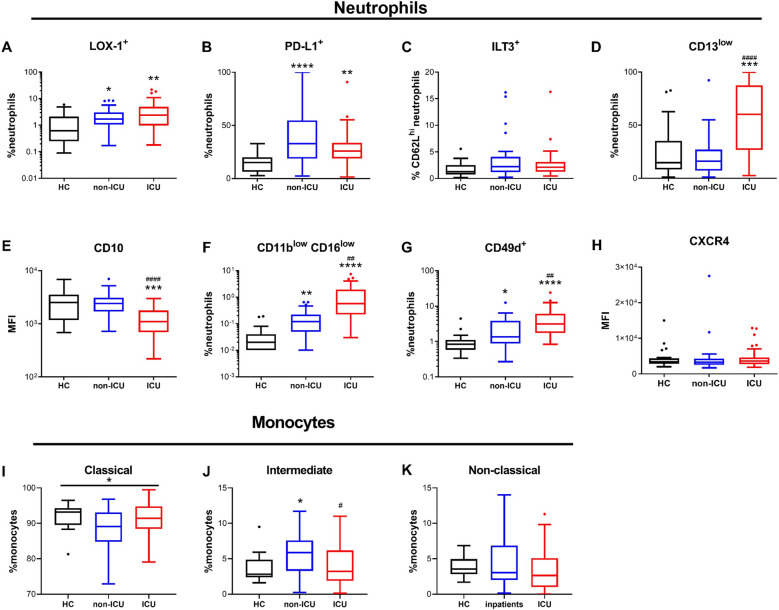
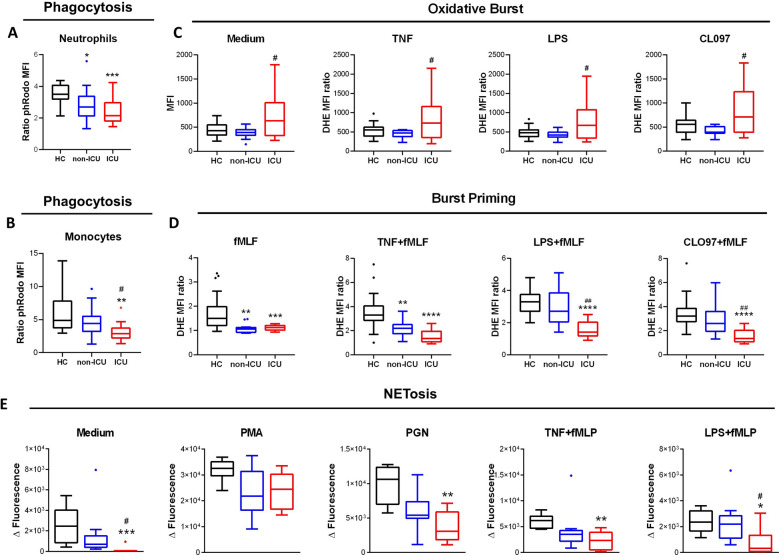
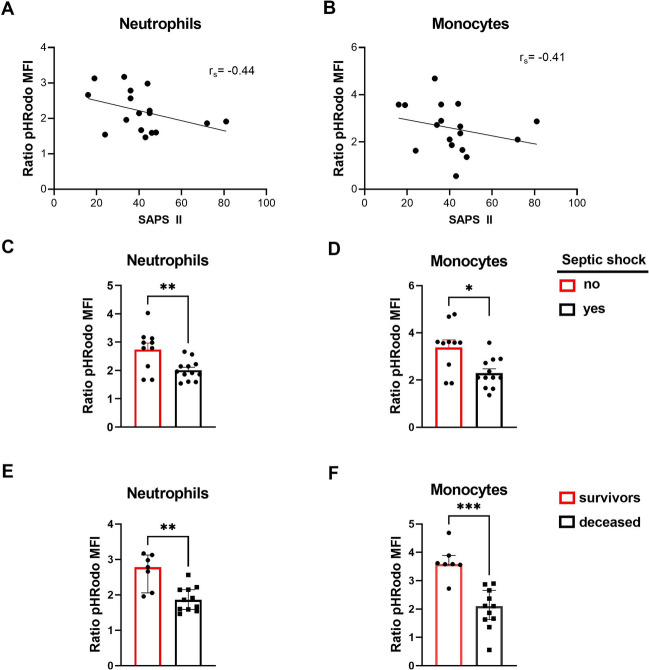
COVID-19 can cause acute respiratory distress syndrome, leading to death in many individuals. Evidence of a deleterious role of the innate immune system is accumulating, but the precise mechanisms involved remain unclear. In this study, we investigated the links between circulating innate phagocytes and severity in COVID-19 patients. We performed in-depth phenotyping of neutrophil and monocyte subpopulations and measured soluble activation markers in plasma. Additionally, anti-microbial functions (phagocytosis, oxidative burst, and NETosis) were evaluated on fresh cells from patients. Neutrophils and monocytes had a strikingly disturbed phenotype, and elevated concentrations of activation markers (calprotectin, myeloperoxidase, and neutrophil extracellular traps) were measured in plasma. Critical patients had increased CD13low immature neutrophils, LOX-1 + and CCR5 + immunosuppressive neutrophils, and HLA-DRlow downregulated monocytes. Markers of immature and immunosuppressive neutrophils were strongly associated with severity. Moreover, neutrophils and monocytes of critical patients had impaired antimicrobial functions, which correlated with organ dysfunction, severe infections, and mortality. Together, our results strongly argue in favor of a pivotal role of innate immunity in COVID-19 severe infections and pleads for targeted therapeutic options.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Sinha P, Matthay MA, Calfee CS. Is a “Cytokine Storm” relevant to COVID-19? JAMA Intern. Med. 2020;180(9):1152–1154. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
