

Delivery Characteristics and the Risk of Early-Onset Neonatal Sepsis
- PMID: 35022750
- PMCID: PMC9648068
- DOI: 10.1542/peds.2021-052900
Delivery Characteristics and the Risk of Early-Onset Neonatal Sepsis
Abstract
Background and objectives: Multiple strategies are used to identify newborn infants at high risk of culture-confirmed early-onset sepsis (EOS). Delivery characteristics have been used to identify preterm infants at lowest risk of infection to guide initiation of empirical antibiotics. Our objectives were to identify term and preterm infants at lowest risk of EOS using delivery characteristics and to determine antibiotic use among them.
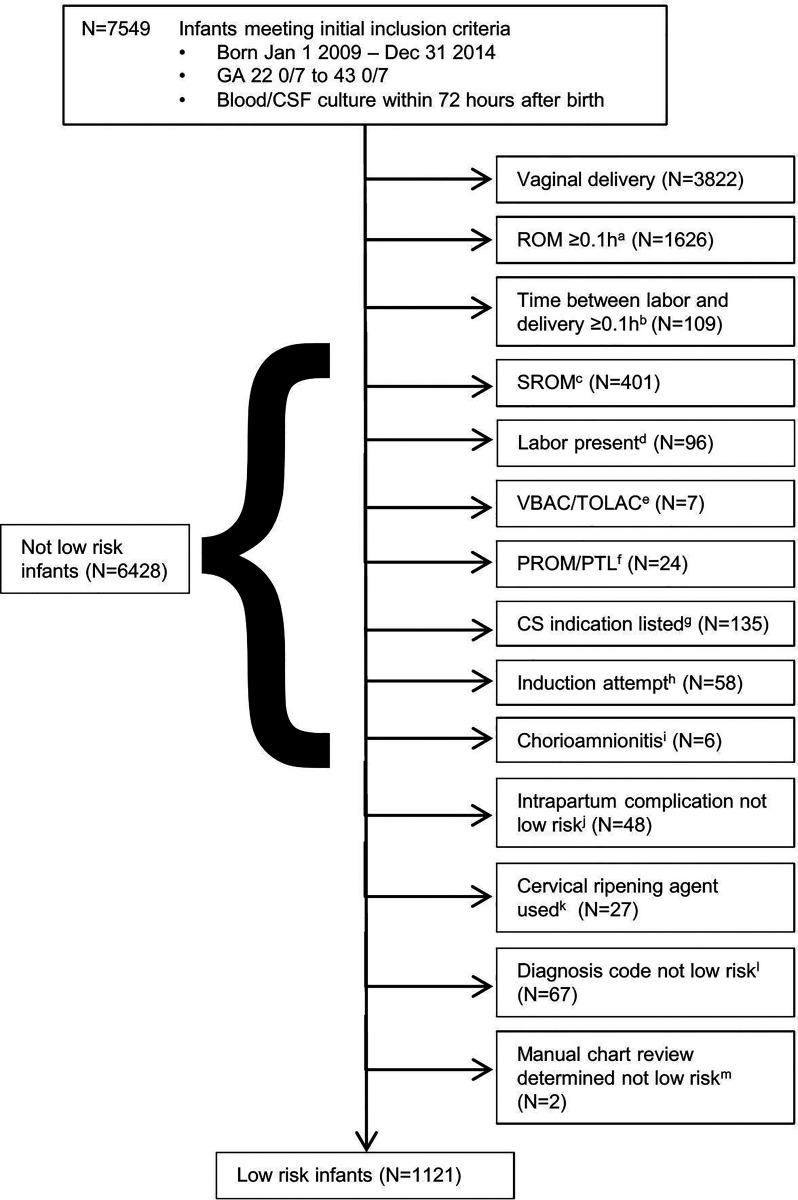
Methods: This was a retrospective cohort study of term and preterm infants born January 1, 2009 to December 31, 2014, with blood culture with or without cerebrospinal fluid culture obtained ≤72 hours after birth. Criteria for determining low EOS risk included: cesarean delivery, without labor or membrane rupture before delivery, and no antepartum concern for intraamniotic infection or nonreassuring fetal status. We determined the association between these characteristics, incidence of EOS, and antibiotic duration among infants without EOS.
Results: Among 53 575 births, 7549 infants (14.1%) were evaluated and 41 (0.5%) of those evaluated had EOS. Low-risk delivery characteristics were present for 1121 (14.8%) evaluated infants, and none had EOS. Whereas antibiotics were initiated in a lower proportion of these infants (80.4% vs 91.0%, P < .001), duration of antibiotics administered to infants born with and without low-risk characteristics was not different (adjusted difference 0.6 hours, 95% CI [-3.8, 5.1]).
Conclusions: Risk of EOS among infants with low-risk delivery characteristics is extremely low. Despite this, a substantial proportion of these infants are administered antibiotics. Delivery characteristics should inform empirical antibiotic management decisions among infants born at all gestational ages.
Copyright © 2022 by the American Academy of Pediatrics.
Conflict of interest statement
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
Figures
Comment in
-
Identifying Neonates at Lowest Risk for Sepsis.Pediatrics. 2022 Feb 1;149(2):e2021054221. doi: 10.1542/peds.2021-054221. Pediatrics. 2022. PMID: 35022789 No abstract available.
-
Low-risk delivery characteristics associated with very low sepsis risk.J Pediatr. 2022 Aug;247:176-180. doi: 10.1016/j.jpeds.2022.04.056. J Pediatr. 2022. PMID: 36058601 No abstract available.
References
-
- Cotten CM, McDonald S, Stoll B, Goldberg RN, Poole K, Benjamin DK Jr; National Institute for Child Health and Human Development Neonatal Research Network . The association of third- generation cephalosporin use and invasive candidiasis in extremely low birth-weight infants. Pediatrics. 2006;118(2):717–722 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
