

Minimally invasive adrenalectomy: a comprehensive systematic review and network meta-analysis of phase II/III randomized clinical controlled trials
- PMID: 35022834
- PMCID: PMC8847275
- DOI: 10.1007/s00423-022-02431-w
Minimally invasive adrenalectomy: a comprehensive systematic review and network meta-analysis of phase II/III randomized clinical controlled trials
Abstract
Purpose: The best approach for minimally invasive adrenalectomy is still under debate.
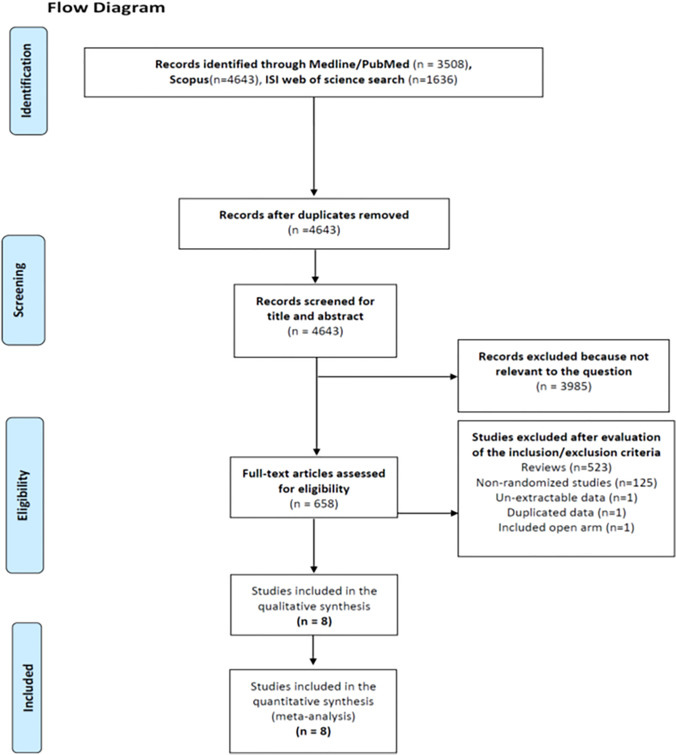
Methods: A systematic search of randomized clinical trials was carried out. A frequentist random-effects network meta-analysis was made reporting the surface under the cumulative ranking (SUCRA). The primary endpoint regarded both in-hospital mortality and morbidity. The secondary endpoints were operative time (OP), blood loss (BL), length of stay (LOS), conversion, incisional hernia, and disease recurrence rate.
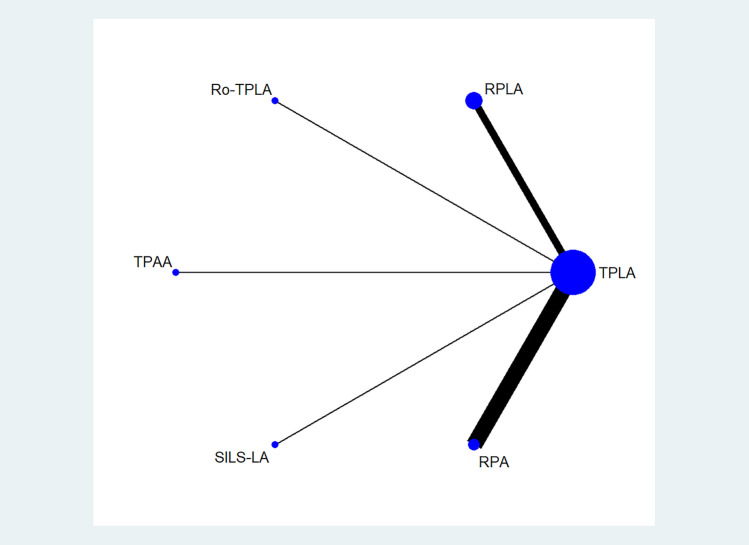
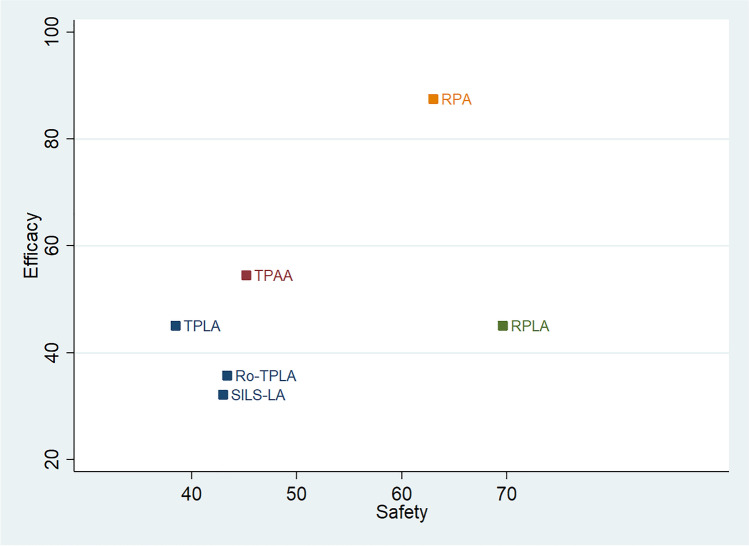
Results: Eight studies were included, involving 359 patients clustered as follows: 175 (48.7%) in the TPLA arm; 55 (15.3%) in the RPLA arm; 10 (2.8%) in the Ro-TPLA arm; 25 (7%) in the TPAA arm; 20 (5.6%) in the SILS-LA arm; and 74 (20.6%) in the RPA arm. The RPLA had the highest probability of being the safest approach (SUCRA 69.6%), followed by RPA (SUCRA 63.0%). TPAA, Ro-TPLA, SILS-LA, and TPLA have similar probability of being safe (SUCRA values 45.2%, 43.4%, 43.0%, and 38.5%, respectively). Analysis of the secondary endpoints confirmed the superiority of RPA regarding OP, BL, LOS, and incisional hernia rate.
Conclusions: The best choice for patients with adrenal masses candidate for minimally invasive surgery seems to be RPA. An alternative could be RPLA. The remaining approaches could have some specific advantages but do not represent the first minimally invasive choice.
Keywords: Efficacy; Laparoscopic adrenalectomy; Network meta-analysis; Retroperitoneal adrenalectomy; Safety.
© 2022. The Author(s).
Conflict of interest statement
All authors disclose financial and non-financial interests that are directly or indirectly related to the work submitted for publication. Finally, all authors disclose any conflict of interests.
Figures
References
-
- Gagner M, Lacroix A, Bolté E. Laparoscopic adrenalectomy in Cushing's syndrome and pheochromocytoma. N Engl J Med. 1992;327(14):1033. - PubMed
-
- Lezoche E, Guerrieri M, Paganini AM, et al. Laparoscopic adrenalectomy by the anterior transperitoneal approach: results of 108 operations in unselected cases. Surg Endosc. 2000;14(10):920–925. - PubMed
-
- Mercan S, Seven R, Ozarmagan S, et al. Endoscopic retroperitoneal adrenalectomy. Surgery. 1995;118(6):1071–5. - PubMed
-
- Walz MK, Alesina PF, Wenger FA, et al. Retroperitoneoscopic adrenalectomy–results of 560 procedures in 520 patients. Surgery. 2006;140(6):943–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
