

Novel Risk Model to Predict Emergency Department Associated Mortality for Patients Supported With a Ventricular Assist Device: The Emergency Department-Ventricular Assist Device Risk Score
- PMID: 35023355
- PMCID: PMC9238533
- DOI: 10.1161/JAHA.121.020942
Novel Risk Model to Predict Emergency Department Associated Mortality for Patients Supported With a Ventricular Assist Device: The Emergency Department-Ventricular Assist Device Risk Score
Abstract
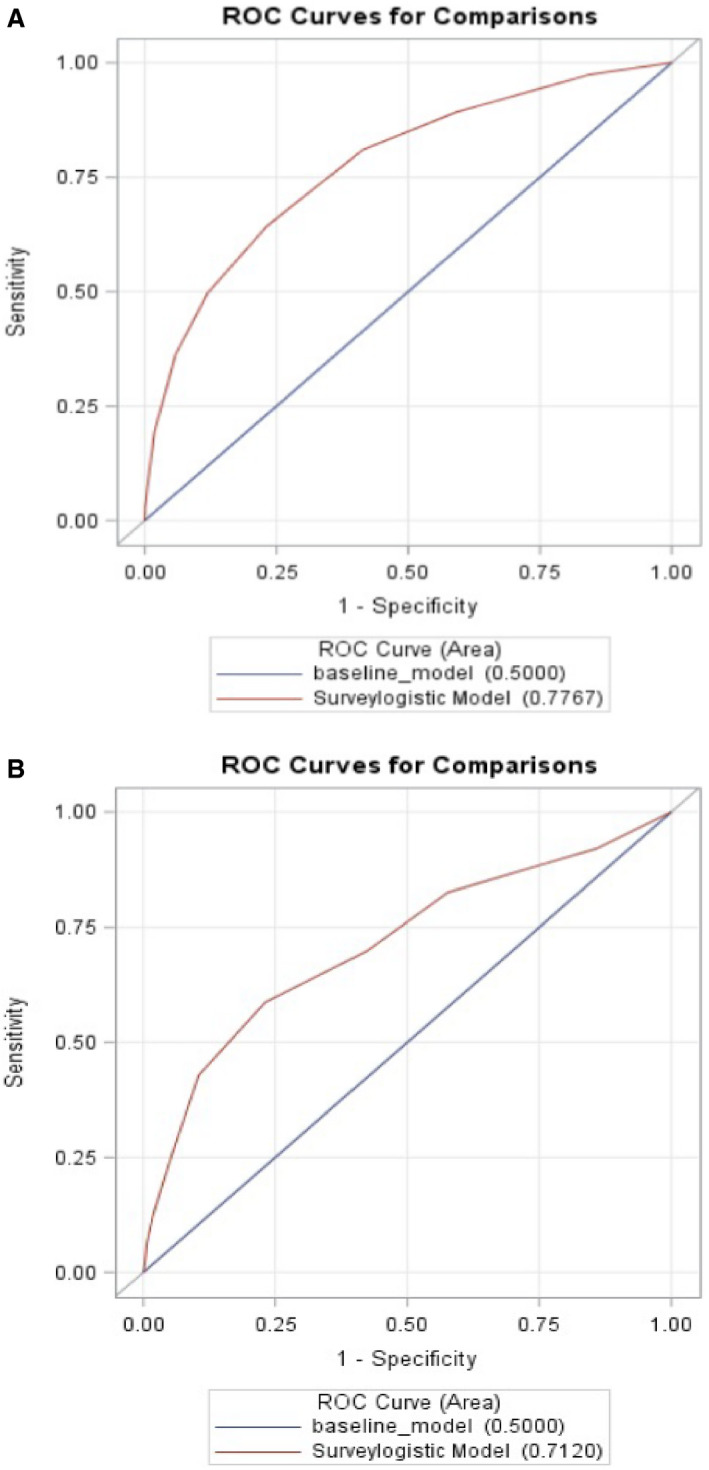
Background The past decade has seen tremendous growth in patients with ambulatory ventricular assist devices. We sought to identify patients that present to the emergency department (ED) at the highest risk of death. Methods and Results This retrospective analysis of ED encounters from the Nationwide Emergency Department Sample includes 2010 to 2017. Using a random sampling of patient encounters, 80% were assigned to development and 20% to validation cohorts. A risk model was derived from independent predictors of mortality. Each patient encounter was assigned to 1 of 3 groups based on risk score. A total of 44 042 ED ventricular assist device patient encounters were included. The majority of patients were male (73.6%), <65 years old (60.1%), and 29% presented with bleeding, stroke, or device complication. Independent predictors of mortality during the ED visit or subsequent admission included age ≥65 years (odds ratio [OR], 1.8; 95% CI, 1.3-4.6), primary diagnoses (stroke [OR, 19.4; 95% CI, 13.1-28.8], device complication [OR, 10.1; 95% CI, 6.5-16.7], cardiac [OR, 4.0; 95% CI, 2.7-6.1], infection [OR, 5.8; 95% CI, 3.5-8.9]), and blood transfusion (OR, 2.6; 95% CI, 1.8-4.0), whereas history of hypertension was protective (OR, 0.69; 95% CI, 0.5-0.9). The risk score predicted mortality areas under the curve of 0.78 and 0.71 for development and validation. Encounters in the highest risk score strata had a 16-fold higher mortality compared with the lowest risk group (15.8% versus 1.0%). Conclusions We present a novel risk score and its validation for predicting mortality of patients with ED ventricular assist devices, a high-risk, and growing, population.
Keywords: mortality; risk score; ventricular assist device.
Figures




Comment in
-
Primary Diagnoses and Relative Risk in Patients With Left Ventricular Assist Devices Visiting an Emergency Department in the United States.J Am Heart Assoc. 2022 Jan 18;11(2):e024228. doi: 10.1161/JAHA.121.024228. Epub 2022 Jan 13. J Am Heart Assoc. 2022. PMID: 35023358 Free PMC article. No abstract available.
References
-
- Teuteberg JJ, Cleveland JC, Cowger J, Higgins RS, Goldstein DJ, Keebler M, Kirklin JK, Myers SL, Salerno CT, Stehlik J, et al. The Society of Thoracic Surgeons Intermacs 2019 Annual Report: the changing landscape of devices and indications. Ann Thorac Surg. 2020;109:649–660. doi: 10.1016/j.athoracsur.2019.12.005 - DOI - PubMed
-
- Edelson JB, Edwards JJ, Katcoff H, Mondal A, Reza N, Hanff TC, Griffis H, Mazurek JA, Wald J, Owens AT, et al. An increasing burden of disease: emergency department visits among patients with ventricular assist devices from 2010–2017. J Am Heart Assoc. 2021;10:e018035. doi: 10.1161/JAHA.120.018035 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
