

Cardiovascular and kidney outcomes with finerenone in patients with type 2 diabetes and chronic kidney disease: the FIDELITY pooled analysis
- PMID: 35023547
- PMCID: PMC8830527
- DOI: 10.1093/eurheartj/ehab777
Cardiovascular and kidney outcomes with finerenone in patients with type 2 diabetes and chronic kidney disease: the FIDELITY pooled analysis
Erratum in
-
Corrigendum to: Cardiovascular and kidney outcomes with finerenone in patients with type 2 diabetes and chronic kidney disease: the FIDELITY pooled analysis.Eur Heart J. 2022 May 21;43(20):1989. doi: 10.1093/eurheartj/ehab886. Eur Heart J. 2022. PMID: 35023545 Free PMC article. No abstract available.
Abstract
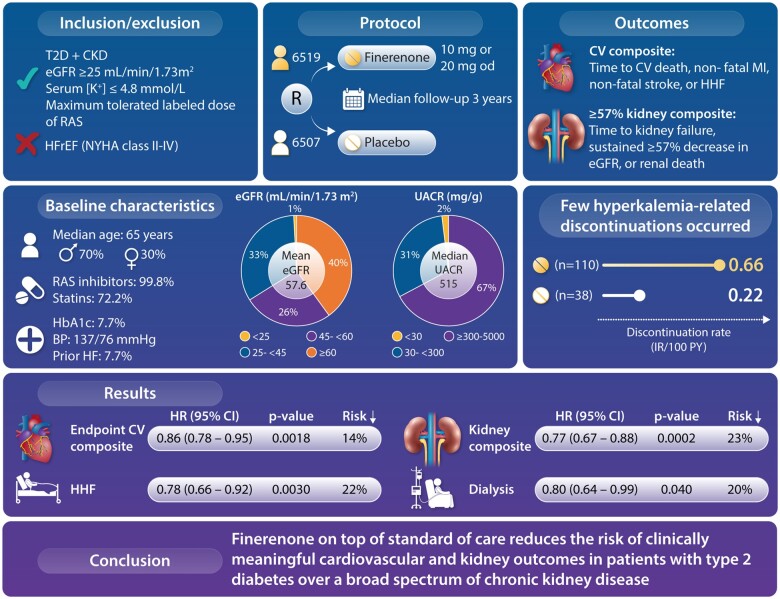
Aims: The complementary studies FIDELIO-DKD and FIGARO-DKD in patients with type 2 diabetes and chronic kidney disease (CKD) examined cardiovascular and kidney outcomes in different, overlapping stages of CKD. The purpose of the FIDELITY analysis was to perform an individual patient-level prespecified pooled efficacy and safety analysis across a broad spectrum of CKD to provide more robust estimates of safety and efficacy of finerenone compared with placebo.
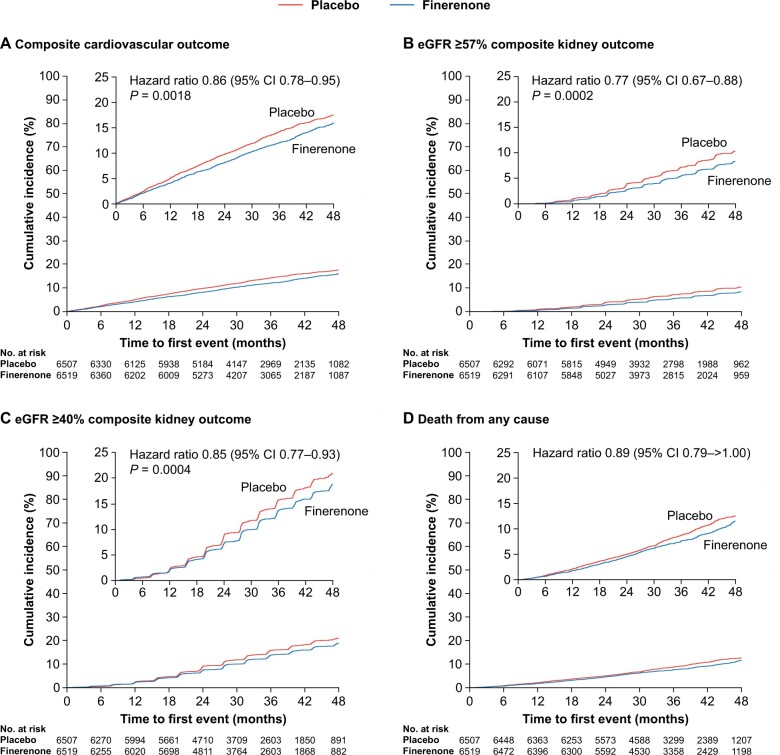
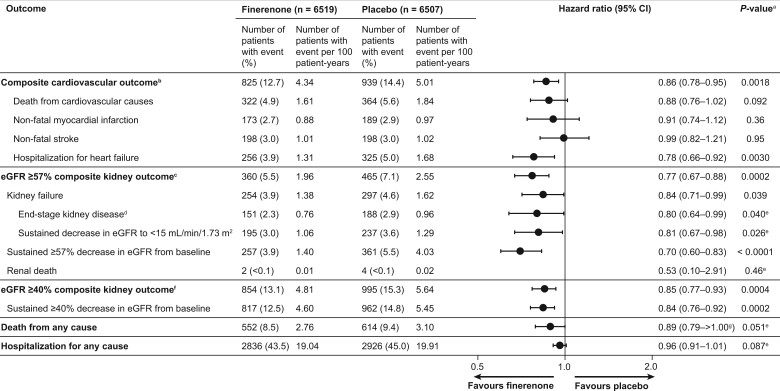
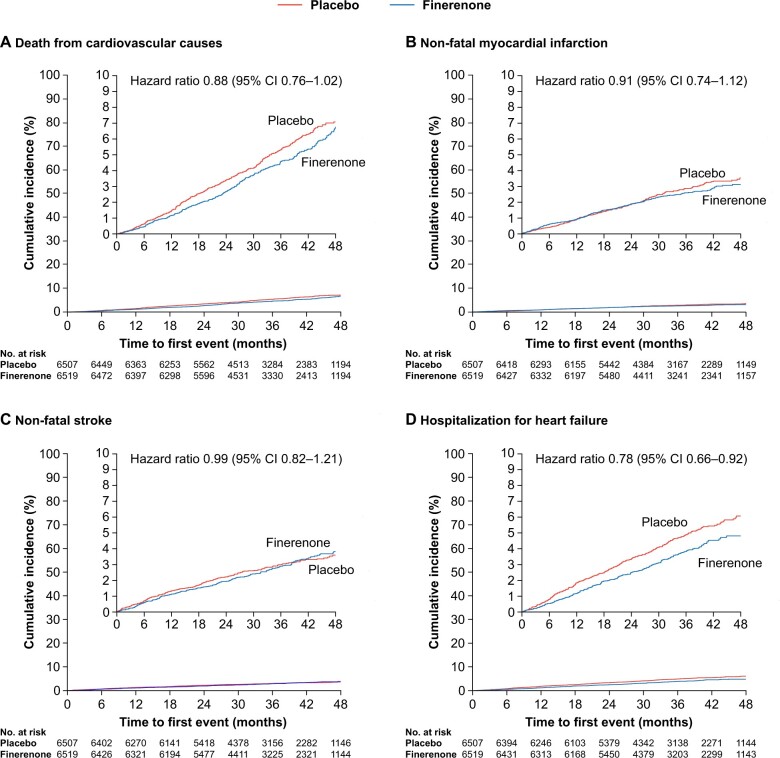
Methods and results: For this prespecified analysis, two phase III, multicentre, double-blind trials involving patients with CKD and type 2 diabetes, randomized 1:1 to finerenone or placebo, were combined. Main time-to-event efficacy outcomes were a composite of cardiovascular death, non-fatal myocardial infarction, non-fatal stroke, or hospitalization for heart failure, and a composite of kidney failure, a sustained ≥57% decrease in estimated glomerular filtration rate from baseline over ≥4 weeks, or renal death. Among 13 026 patients with a median follow-up of 3.0 years (interquartile range 2.3-3.8 years), the composite cardiovascular outcome occurred in 825 (12.7%) patients receiving finerenone and 939 (14.4%) receiving placebo [hazard ratio (HR), 0.86; 95% confidence interval (CI), 0.78-0.95; P = 0.0018]. The composite kidney outcome occurred in 360 (5.5%) patients receiving finerenone and 465 (7.1%) receiving placebo (HR, 0.77; 95% CI, 0.67-0.88; P = 0.0002). Overall safety outcomes were generally similar between treatment arms. Hyperkalaemia leading to permanent treatment discontinuation occurred more frequently in patients receiving finerenone (1.7%) than placebo (0.6%).
Conclusion: Finerenone reduced the risk of clinically important cardiovascular and kidney outcomes vs. placebo across the spectrum of CKD in patients with type 2 diabetes.
Key question: Does finerenone, a novel selective, nonsteroidal mineralocorticoid receptor antagonist, added to maximum tolerated renin-angiotensin system inhibition reduce cardiovascular disease and kidney disease progression over a broad range of chronic kidney disease in patients with type 2 diabetes?
Key finding: In a prespecified, pooled individual-level analysis from two randomized trials, we found reductions both in cardiovascular events and kidney failure outcomes with finerenone. Because 40% of the patients had an estimated glomerular filtration rate of >60 mL/min/1.73m2 they were identified solely on the basis of albuminuria.
Take home message: Finerenone reduces the risk of clinical cardiovascular outcomes and kidney disease progression in a broad range of patients with chronic kidney disease and type 2 diabetes. Screening for albuminuria to identify at-risk patients among patients with type 2 diabetes facilitates reduction of both cardiovascular and kidney disease burden.
Keywords: Cardiorenal outcomes; Chronic kidney disease; Finerenone; Hospitalization for heart failure; Hyperkalaemia; Type 2 diabetes.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Bringing FIDELITY to the estimate of treatment effects of finerenone in chronic kidney disease due to type 2 diabetes.Eur Heart J. 2022 Feb 10;43(6):485-487. doi: 10.1093/eurheartj/ehab827. Eur Heart J. 2022. PMID: 34888636 No abstract available.
-
In patients with type 2 diabetes and CKD, finerenone improved CV and kidney outcomes.Ann Intern Med. 2022 May;175(5):JC54. doi: 10.7326/J22-0029. Epub 2022 May 3. Ann Intern Med. 2022. PMID: 35500259
-
Die dritte Säule der organprotektiven Therapie.MMW Fortschr Med. 2023 Apr;165(8):57. doi: 10.1007/s15006-023-2565-0. MMW Fortschr Med. 2023. PMID: 37081358 German. No abstract available.
References
-
- Perkovic V, Jardine MJ, Neal B et al.; CREDENCE Trial Investigators. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med 2019;380:2295–2306. - PubMed
-
- Neuen BL, Young T, Heerspink HJL et al. SGLT2 inhibitors for the prevention of kidney failure in patients with type 2 diabetes: a systematic review and meta-analysis. Lancet Diabetes Endocrinol 2019;7:845–854. - PubMed
-
- Zelniker TA, Wiviott SD, Raz I et al. Comparison of the effects of glucagon-like peptide receptor agonists and sodium-glucose cotransporter 2 inhibitors for prevention of major adverse cardiovascular and renal outcomes in type 2 diabetes mellitus. Circulation 2019;139:2022–2031. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
