

Impact of 1-hour and 3-hour sepsis time bundles on patient outcomes and antimicrobial use: A before and after cohort study
- PMID: 35024649
- PMCID: PMC8654968
- DOI: 10.1016/j.lanwpc.2021.100305
Impact of 1-hour and 3-hour sepsis time bundles on patient outcomes and antimicrobial use: A before and after cohort study
Abstract
Background: Sepsis bundles, promulgated by Surviving Sepsis Campaign have not been widely adopted because of variability in sepsis identification strategies, implementation challenges, concerns about excess antimicrobial use, and limited evidence of benefit.
Methods: A 1-hour septic shock and a 3-hour sepsis bundle were implemented using a Breakthrough Series Collaborative in 14 public hospitals in Queensland, Australia. A before (baseline) and after (post-intervention) study evaluated its impact on outcomes and antimicrobial prescription in patients with confirmed bacteremia and sepsis.
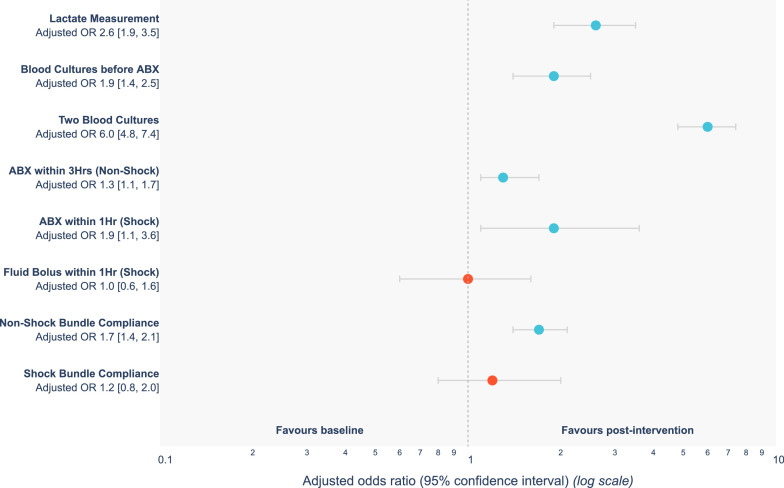
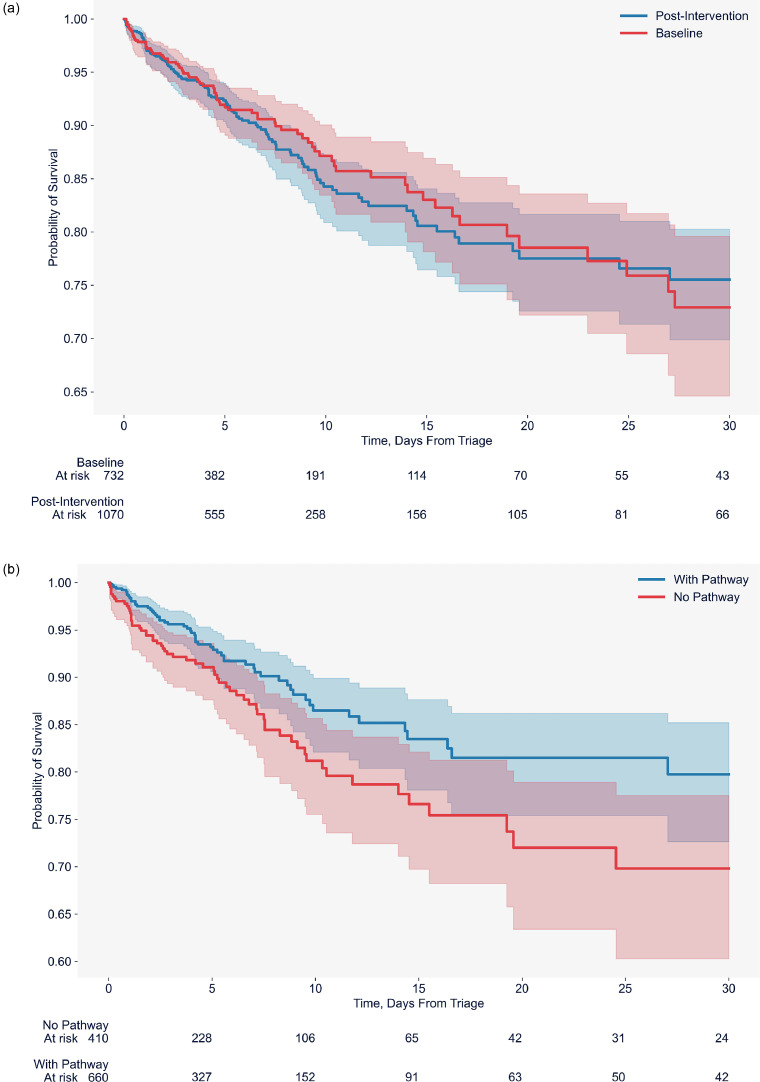
Findings: Between 01 July 2017 to 31 March 2020, of 6976 adults presenting to the Emergency Departments and had a blood culture taken, 1802 patients (732 baseline, 1070 post-intervention) met inclusion criteria. Time to antibiotics in 1-hour 73.7% vs 85.1% (OR 1.9 [95%CI 1.1-3.6]) and the 3-hour bundle compliance (48.2% to 63.3%, OR 1.7, [95%CI 1.4 to 2.1]) improved post-intervention, accompanied by a significant reduction in Intensive Care Unit (ICU) admission rates (26.5% vs 17.5% (OR 0.5, [95%CI 0.4 to 0.7]). There were no significant differences in-hospital and 30-day post discharge mortality between the two phases. In a post-hoc analysis of the post-intervention phase, sepsis pathway compliance was associated with lower in-hospital mortality (9.7% vs 14.9%, OR 0.6, 95%CI 0.4 to 0.8). The proportions of appropriate antimicrobial prescription at baseline and post-intervention respectively were 55.4% vs 64.1%, (OR 1.4 [95%CI 0.9 to 2.1]).
Interpretation: Implementing 1-hour and 3-hour sepsis bundles for patients presenting with bacteremia resulted in improved bundle compliance and a reduced need for ICU admission without adversely influencing antimicrobial prescription.
© 2021 The Authors.
Conflict of interest statement
None
Figures
References
-
- Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive care med. 2017;43:304–377. - PubMed
-
- Rhodes A, Phillips G, Beale R. al.The Surviving Sepsis Campaign bundles and outcome: results from the International Multicentre Prevalence Study on Sepsis (the IMPreSS study) Intensive Care Med. 2015;41:1620–1628. - PubMed
-
- Levy MM, Evans LE, Rhodes A. The Surviving Sepsis Campaign Bundle: 2018 update. Intensive Care Medicine. 2018;44:925–928. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
