

Antibiotic use for empirical therapy in the critical care units in primary and secondary hospitals in Vietnam: a multicenter cross-sectional study
- PMID: 35024650
- PMCID: PMC8669321
- DOI: 10.1016/j.lanwpc.2021.100306
Antibiotic use for empirical therapy in the critical care units in primary and secondary hospitals in Vietnam: a multicenter cross-sectional study
Abstract
Background: The high rate of infections among patients admitted to critical care units (CCUs) is associated with high rate of antibiotic consumption, especially broad-spectrum antibiotics. This study is to describe the antibiotics use in CCUs in primary and secondary hospitals in Vietnam, a setting with high burden of antibiotic resistance.
Methods: This was a 7-day observational study in 51 CCUs in hospitals from 5 provinces in Vietnam from March to July 2019. Patients aged ≥ 18 years admitted to the participating CCUs was enrolled consecutively. We collected data on patient's demographics, initial diagnosis and antibiotic therapy within the first 24 hours. Antibiotic therapy was classified by the Anatomical Therapeutic Chemical (ATC) Index and the 2019 WHO Access, Watch, Reserve (AWaRe) groups.
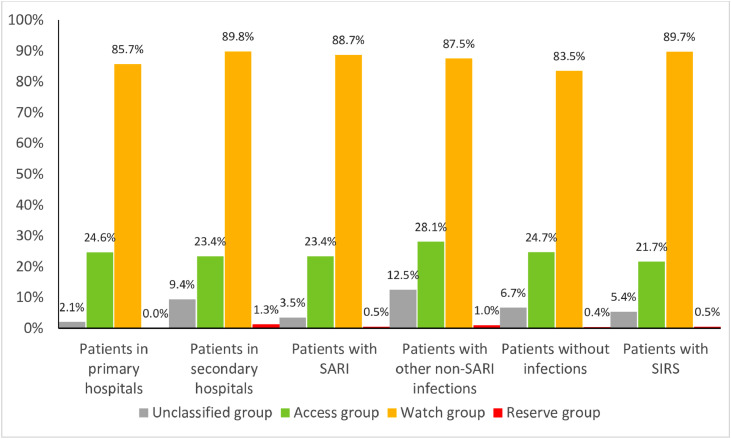
Findings: Out of 1747 enrolled patients, empirical antibiotic treatments were initiated in 1112 (63.6%) patients. The most frequently prescribed antibiotics were cefotaxime (22.3%), levofloxacin (19%) and ceftazidime (10.8%). Antibiotics were given in 31.5% of patients without diagnosis of infection. Watch and/or Reserve group antibiotic were given in 87.3% of patients and associated with patient's age (aOR 1.01 per 1-year increment, 95%CI 1.00-1.02) and the presence of SIRS on admission (aOR 2.1, 95%CI 1.38-3.2).
Interpretation: We observed a high frequency use and a substantial variation in patterns of empirical antibiotic use in the CCUs in Vietnam. It highlights the importance of continuous monitoring antibiotic consumption in CCUs.
Keywords: AWaRe; antibiotic; antimicrobials; critical care; emergency; infection, ICD-10; sepsis; severe acute respiratory.
© 2021 The Authors.
Conflict of interest statement
We declare no competing interest.
Figures
References
-
- GBD 2017 Lower Respiratory Infections Collaborators Estimates of the global, regional, and national morbaidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect Dis. 2018;18(11):1191–1210. - PMC - PubMed
-
- Fleischmann C., Scherag A., Adhikari N.K., Hartog C.S., Tsaganos T., Schlattmann P., et al. Assessment of Global Incidence and Mortality of Hospital-treated Sepsis. Current Estimates and Limitations. American journal of respiratory and critical care medicine. 2016;193(3):259–272. - PubMed
-
- Bassetti M., Rello J., Blasi F., Goossens H., Sotgiu G., Tavoschi L., et al. Systematic review of the impact of appropriate versus inappropriate initial antibiotic therapy on outcomes of patients with severe bacterial infections. International journal of antimicrobial agents. 2020;56(6) - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
