

Characteristics and outcome of COVID-19 patients admitted to the ICU: a nationwide cohort study on the comparison between the first and the consecutive upsurges of the second wave of the COVID-19 pandemic in the Netherlands
- PMID: 35024981
- PMCID: PMC8755895
- DOI: 10.1186/s13613-021-00978-3
Characteristics and outcome of COVID-19 patients admitted to the ICU: a nationwide cohort study on the comparison between the first and the consecutive upsurges of the second wave of the COVID-19 pandemic in the Netherlands
Abstract
Background: To assess trends in the quality of care for COVID-19 patients at the ICU over the course of time in the Netherlands.
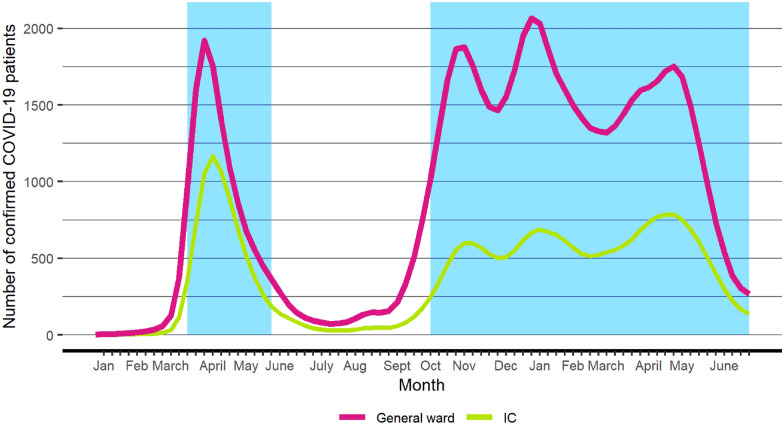
Methods: Data from the National Intensive Care Evaluation (NICE)-registry of all COVID-19 patients admitted to an ICU in the Netherlands were used. Patient characteristics and indicators of quality of care during the first two upsurges (N = 4215: October 5, 2020-January 31, 2021) and the final upsurge of the second wave, called the 'third wave' (N = 4602: February 1, 2021-June 30, 2021) were compared with those during the first wave (N = 2733, February-May 24, 2020).
Results: During the second and third wave, there were less patients treated with mechanical ventilation (58.1 and 58.2%) and vasoactive drugs (48.0 and 44.7%) compared to the first wave (79.1% and 67.2%, respectively). The occupancy rates as fraction of occupancy in 2019 (1.68 and 1.55 vs. 1.83), the numbers of ICU relocations (23.8 and 27.6 vs. 32.3%) and the mean length of stay at the ICU (HRs of ICU discharge = 1.26 and 1.42) were lower during the second and third wave. No difference in adjusted hospital mortality between the second wave and the first wave was found, whereas the mortality during the third wave was considerably lower (OR = 0.80, 95% CI [0.71-0.90]).
Conclusions: These data show favorable shifts in the treatment of COVID-19 patients at the ICU over time. The adjusted mortality decreased in the third wave. The high ICU occupancy rate early in the pandemic does probably not explain the high mortality associated with COVID-19.
Keywords: COVID-19; Coronavirus; Critical Care; Intensive Care; Mortality; Outcome.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Richards-Belle A, Orzechowska I, Gould DW, Thomas K, Doidge JC, Mouncey PR, Christian MD, Shankar-Hari M, Harrison DA, Rowan KM, ICNARC COVID-19 Team COVID-19 in critical care: epidemiology of the first pandemic wave across England, Wales and Northern Ireland. Intensive Care Med. 2020;46(11):2035–2047. doi: 10.1007/s00134-020-06267-0. - DOI - PMC - PubMed
-
- Albrecht R, Knapp J, Theiler L, Eder M, Pietsch U. Transport of COVID-19 and other highly contagious patients by helicopter and fixed-wing air ambulance: a narrative review and experience of the Swiss air rescue Rega. Scand J Trauma Resusc Emerg Med. 2020;28(1):40. doi: 10.1186/s13049-020-00734-9. - DOI - PMC - PubMed
-
- Janz DR, Khan YA, Mooney JL, Semler MW, Rice TW, Johnson JL, deBoisblanc BP, ICU MOVE Investigators and the Pragmatic Critical Care Research Group Effect of interhospital ICU relocation on patient physiology and clinical outcomes. J Intensive Care Med. 2019;34(11–12):1010–1016. doi: 10.1177/0885066617726754. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
