

Mutant PPM1D- and TP53-Driven Hematopoiesis Populates the Hematopoietic Compartment in Response to Peptide Receptor Radionuclide Therapy
- PMID: 35025619
- PMCID: PMC8769150
- DOI: 10.1200/PO.21.00309
Mutant PPM1D- and TP53-Driven Hematopoiesis Populates the Hematopoietic Compartment in Response to Peptide Receptor Radionuclide Therapy
Abstract
Purpose: Hematologic toxic effects of peptide receptor radionuclide therapy (PRRT) can be permanent. Patients with underlying clonal hematopoiesis (CH) may be more inclined to develop hematologic toxicity after PRRT. However, this association remains understudied.
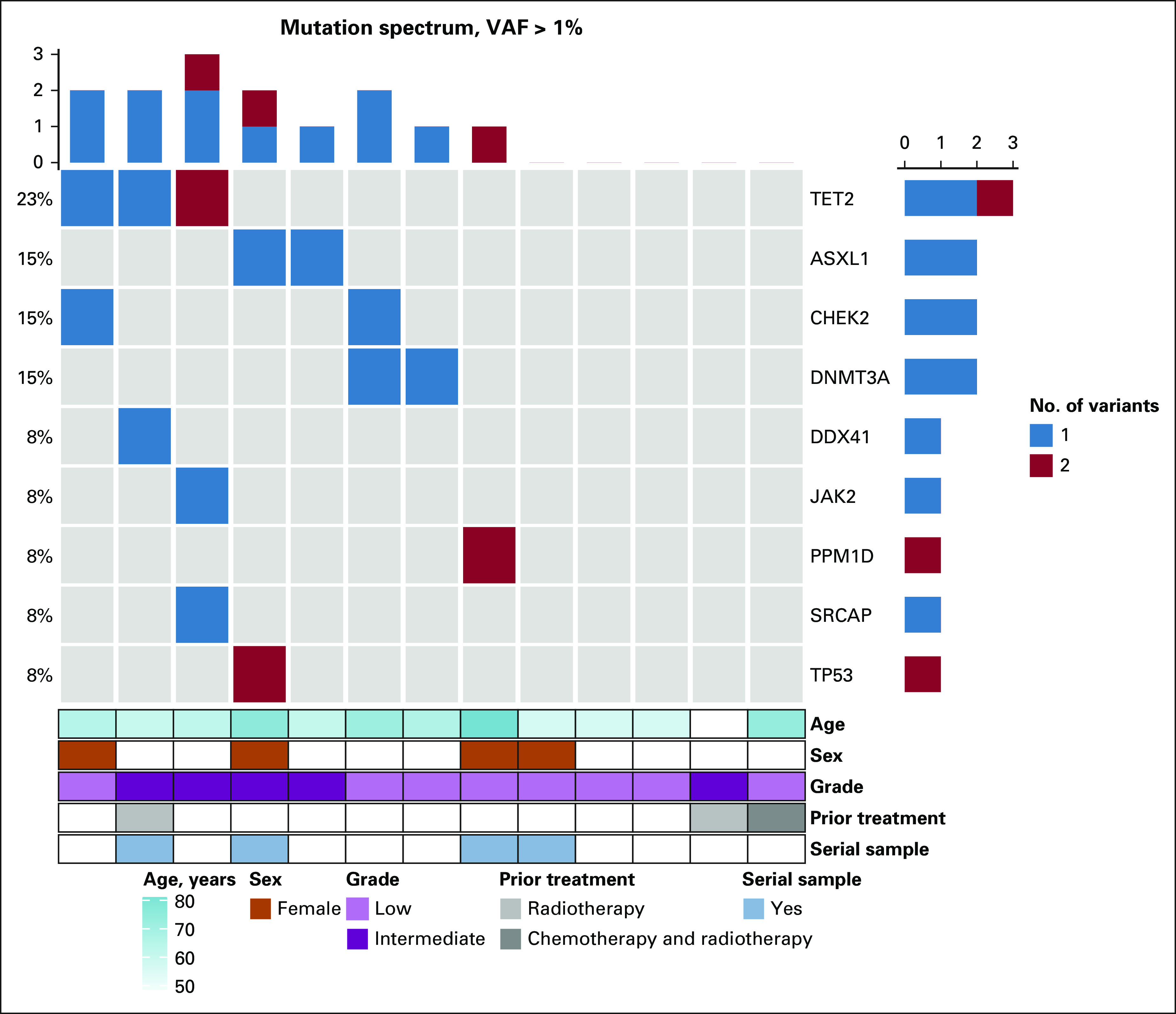
Materials and methods: We evaluated pre- and post-PRRT blood samples of patients with neuroendocrine tumors. After initial screening, 13 cases of interest were selected. Serial blood samples were obtained on 4 of 13 patients. Genomic DNA was analyzed using a 100-gene panel. A variant allele frequency cutoff of 1% was used to call CH.
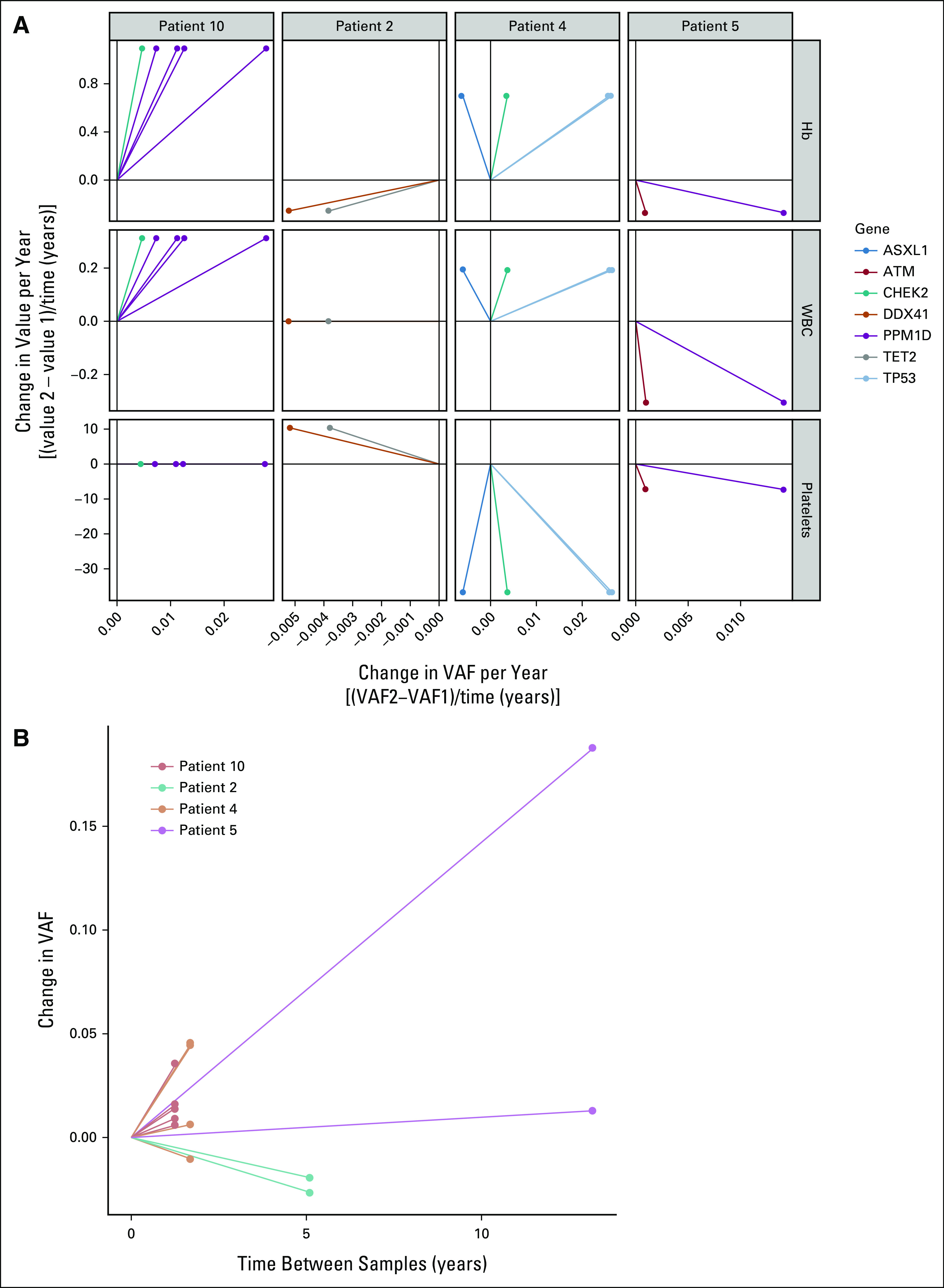
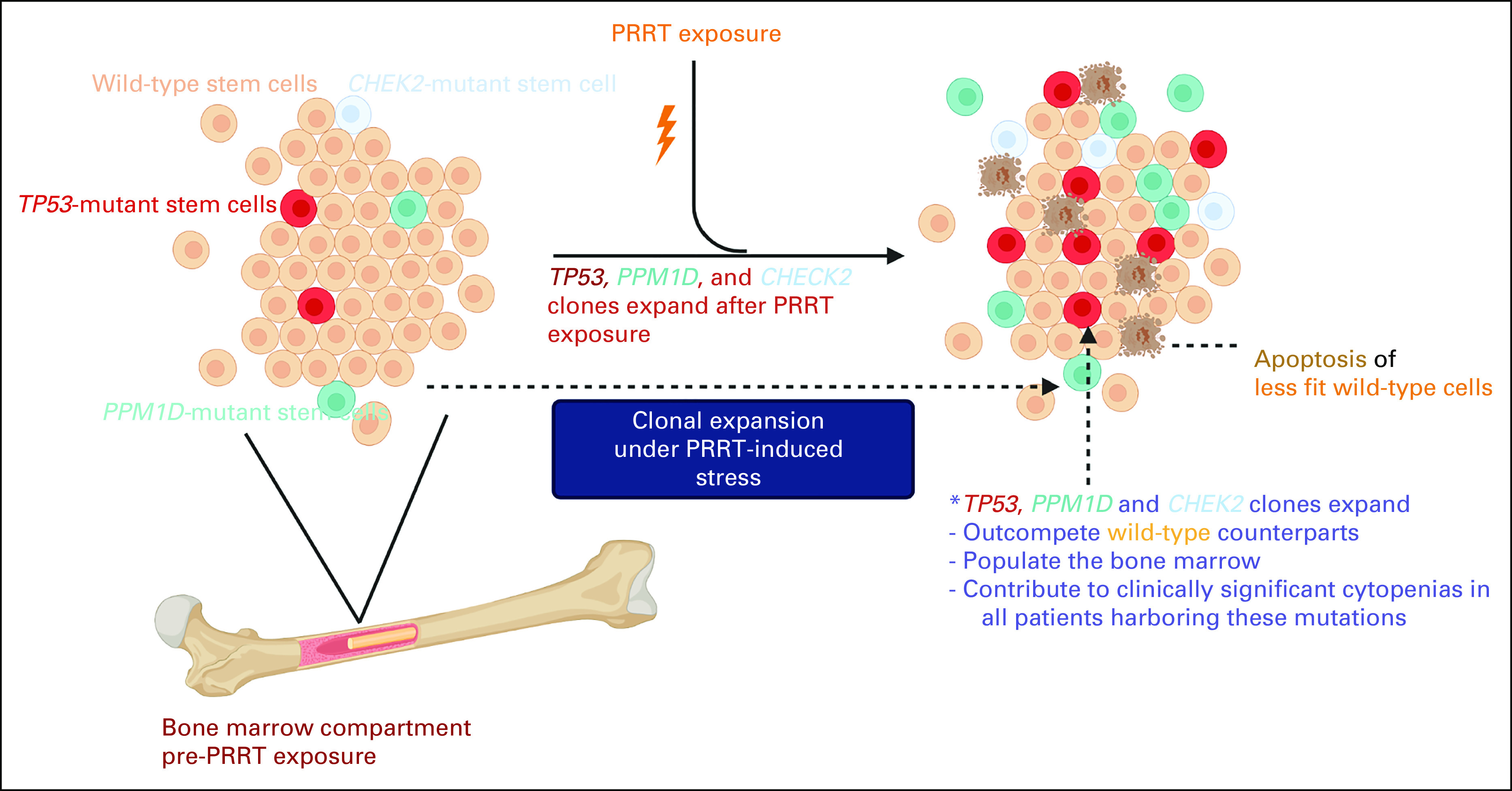
Result: Sixty-two percent of patients had CH at baseline. Persistent cytopenias were noted in 64% (7 of 11) of the patients. Serial sample analysis demonstrated that PRRT exposure resulted in clonal expansion of mutant DNA damage response genes (TP53, CHEK2, and PPM1D) and accompanying cytopenias in 75% (3 of 4) of the patients. One patient who had a normal baseline hemogram and developed persistent cytopenias after PRRT exposure showed expansion of mutant PPM1D (variant allele frequency increased to 20% after exposure from < 1% at baseline). In the other two patients, expansion of mutant TP53, CHEK2, and PPM1D clones was also noted along with cytopenia development.
Conclusion: The shifts in hematopoietic clonal dynamics in our study were accompanied by emergence and persistence of cytopenias. These cytopenias likely represent premalignant state, as PPM1D-, CHEK2-, and TP53-mutant clones by themselves carry a high risk for transformation to therapy-related myeloid neoplasms. Future studies should consider CH screening and longitudinal monitoring as a key risk mitigation strategy for patients with neuroendocrine tumors receiving PRRT.
Conflict of interest statement
Figures
References
-
- American Cancer Society : Facts & figures 2020 reports largest one-year drop in cancer mortality, 2020. https://www.cancer.org/latest-news/facts-and-figures-2020.html
-
- Granfeldt Ostgard LS, Medeiros BC, Sengelov H, et al. : Epidemiology and clinical significance of secondary and therapy-related acute myeloid leukemia: A national population-based cohort study. J Clin Oncol 33:3641-3649, 2015 - PubMed
-
- Chung J, Sallman DA, Padron E: TP53 and therapy-related myeloid neoplasms. Best Pract Res Clin Haematol 32:98-103, 2019 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
