

Risk for Newly Diagnosed Diabetes >30 Days After SARS-CoV-2 Infection Among Persons Aged <18 Years - United States, March 1, 2020-June 28, 2021
- PMID: 35025851
- PMCID: PMC8757617
- DOI: 10.15585/mmwr.mm7102e2
Risk for Newly Diagnosed Diabetes >30 Days After SARS-CoV-2 Infection Among Persons Aged <18 Years - United States, March 1, 2020-June 28, 2021
Abstract
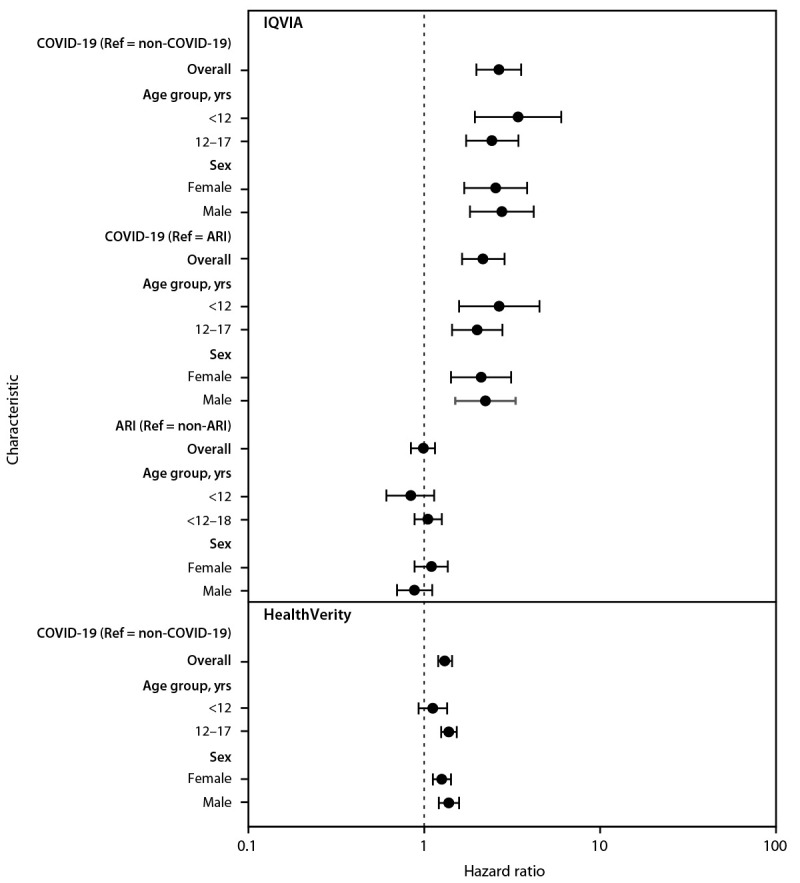
The COVID-19 pandemic has disproportionately affected people with diabetes, who are at increased risk of severe COVID-19.* Increases in the number of type 1 diabetes diagnoses (1,2) and increased frequency and severity of diabetic ketoacidosis (DKA) at the time of diabetes diagnosis (3) have been reported in European pediatric populations during the COVID-19 pandemic. In adults, diabetes might be a long-term consequence of SARS-CoV-2 infection (4-7). To evaluate the risk for any new diabetes diagnosis (type 1, type 2, or other diabetes) >30 days† after acute infection with SARS-CoV-2 (the virus that causes COVID-19), CDC estimated diabetes incidence among patients aged <18 years (patients) with diagnosed COVID-19 from retrospective cohorts constructed using IQVIA health care claims data from March 1, 2020, through February 26, 2021, and compared it with incidence among patients matched by age and sex 1) who did not receive a COVID-19 diagnosis during the pandemic, or 2) who received a prepandemic non-COVID-19 acute respiratory infection (ARI) diagnosis. Analyses were replicated using a second data source (HealthVerity; March 1, 2020-June 28, 2021) that included patients who had any health care encounter possibly related to COVID-19. Among these patients, diabetes incidence was significantly higher among those with COVID-19 than among those 1) without COVID-19 in both databases (IQVIA: hazard ratio [HR] = 2.66, 95% CI = 1.98-3.56; HealthVerity: HR = 1.31, 95% CI = 1.20-1.44) and 2) with non-COVID-19 ARI in the prepandemic period (IQVIA, HR = 2.16, 95% CI = 1.64-2.86). The observed increased risk for diabetes among persons aged <18 years who had COVID-19 highlights the importance of COVID-19 prevention strategies, including vaccination, for all eligible persons in this age group,§ in addition to chronic disease prevention and management. The mechanism of how SARS-CoV-2 might lead to incident diabetes is likely complex and could differ by type 1 and type 2 diabetes. Monitoring for long-term consequences, including signs of new diabetes, following SARS-CoV-2 infection is important in this age group.
Conflict of interest statement
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. No potential conflicts of interest were disclosed.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
