

Clinical Opinion: The diagnosis and management of suspected fetal growth restriction: an evidence-based approach
- PMID: 35026129
- PMCID: PMC9125563
- DOI: 10.1016/j.ajog.2021.11.1357
Clinical Opinion: The diagnosis and management of suspected fetal growth restriction: an evidence-based approach
Abstract
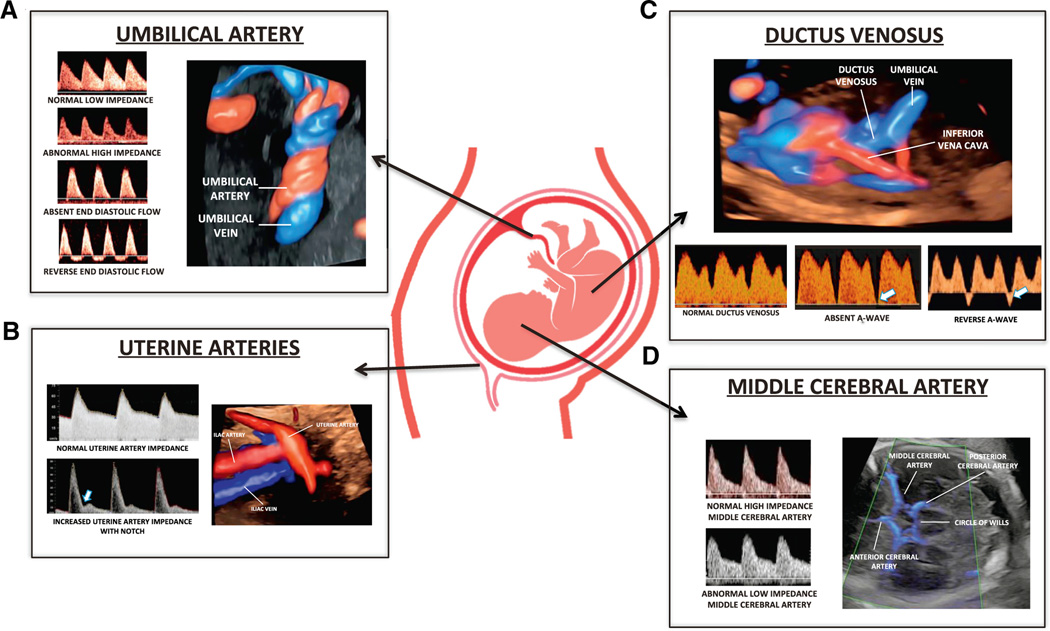
This study reviewed the literature about the diagnosis, antepartum surveillance, and time of delivery of fetuses suspected to be small for gestational age or growth restricted. Several guidelines have been issued by major professional organizations, including the International Society of Ultrasound in Obstetrics and Gynecology and the Society for Maternal-Fetal Medicine. The differences in recommendations, in particular about Doppler velocimetry of the ductus venosus and middle cerebral artery, have created confusion among clinicians, and this review has intended to clarify and highlight the available evidence that is pertinent to clinical management. A fetus who is small for gestational age is frequently defined as one with an estimated fetal weight of <10th percentile. This condition has been considered syndromic and has been frequently attributed to fetal growth restriction, a constitutionally small fetus, congenital infections, chromosomal abnormalities, or genetic conditions. Small for gestational age is not synonymous with fetal growth restriction, which is defined by deceleration of fetal growth determined by a change in fetal growth velocity. An abnormal umbilical artery Doppler pulsatility index reflects an increased impedance to flow in the umbilical circulation and is considered to be an indicator of placental disease. The combined finding of an estimated fetal weight of <10th percentile and abnormal umbilical artery Doppler velocimetry has been widely accepted as indicative of fetal growth restriction. Clinical studies have shown that the gestational age at diagnosis can be used to subclassify suspected fetal growth restriction into early and late, depending on whether the condition is diagnosed before or after 32 weeks of gestation. The early type is associated with umbilical artery Doppler abnormalities, whereas the late type is often associated with a low pulsatility index in the middle cerebral artery. A large randomized clinical trial indicated that in the context of early suspected fetal growth restriction, the combination of computerized cardiotocography and fetal ductus venosus Doppler improves outcomes, such that 95% of surviving infants have a normal neurodevelopmental outcome at 2 years of age. A low middle cerebral artery pulsatility index is associated with an adverse perinatal outcome in late fetal growth restriction; however, there is no evidence supporting its use to determine the time of delivery. Nonetheless, an abnormality in middle cerebral artery Doppler could be valuable to increase the surveillance of the fetus at risk. We propose that fetal size, growth rate, uteroplacental Doppler indices, cardiotocography, and maternal conditions (ie, hypertension) according to gestational age are important factors in optimizing the outcome of suspected fetal growth restriction.
Keywords: Disproportionate Intrauterine Growth Intervention Trial at Term; Doppler velocimetry; Prospective Observational Trial to Optimize Pediatric Health; Trial of Umbilical and Fetal Flow in Europe; abdominal circumference; cardiotocography; cesarean delivery; ductus venosus; fetal biometry; fetal death; fetal distress; fetal growth; longitudinal; middle cerebral artery; neurodevelopmental outcome; randomized controlled trial; short-term variation; small for gestational age; systematic review; umbilical artery Doppler; umbilical artery pH; uterine artery.
Copyright © 2022. Published by Elsevier Inc.
Conflict of interest statement
The other authors report no conflict of interest.
Figures





References
-
- McCowan LM, Figueras F, Anderson NH. Evidence-based national guidelines for the management of suspected fetal growth restriction: comparison, consensus, and controversy. Am J Obstet Gynecol 2018;218:S855–68. - PubMed
-
- Chauhan SP, Gupta LM, Hendrix NW, Berghella V; American College of Obstetricians and Gynecologists. Intrauterine growth restriction: comparison of American College of Obstetricians and Gynecologists practice bulletin with other national guidelines. Am J Obstet Gynecol 2009;200:409.e1–6. - PubMed
-
- Society for Maternal-Fetal Medicine, Martins JG, Biggio JR, Abuhamad A. Society for Maternal-Fetal Medicine Consult Series #52: diagnosis and management of fetal growth restriction: (replaces clinical guideline number 3, April 2012). Am J Obstet Gynecol 2020;223: B2–17. - PubMed
-
- Lees CC, Stampalija T, Baschat A, et al. ISUOG Practice Guidelines: diagnosis and management of small-for-gestational-age fetus and fetal growth restriction. Ultrasound Obstet Gynecol 2020;56:298–312. - PubMed
-
- Gordijn SJ, Beune IM, Thilaganathan B, et al. Consensus definition of fetal growth restriction: a Delphi procedure. Ultrasound Obstet Gynecol 2016;48:333–9. - PubMed
