

Long-term perturbation of the peripheral immune system months after SARS-CoV-2 infection
- PMID: 35027067
- PMCID: PMC8758383
- DOI: 10.1186/s12916-021-02228-6
Long-term perturbation of the peripheral immune system months after SARS-CoV-2 infection
Abstract
Background: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a highly infectious respiratory virus which is responsible for the coronavirus disease 2019 (COVID-19) pandemic. It is increasingly clear that recovered individuals, even those who had mild COVID-19, can suffer from persistent symptoms for many months after infection, a condition referred to as "long COVID", post-acute sequelae of COVID-19 (PASC), post-acute COVID-19 syndrome, or post COVID-19 condition. However, despite the plethora of research on COVID-19, relatively little is known about the molecular underpinnings of these long-term effects.
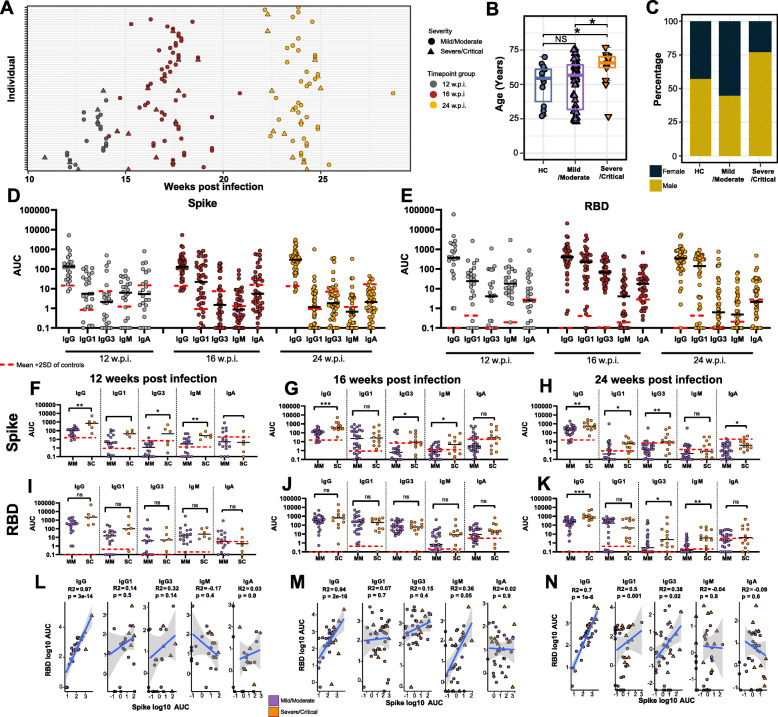
Methods: We have undertaken an integrated analysis of immune responses in blood at a transcriptional, cellular, and serological level at 12, 16, and 24 weeks post-infection (wpi) in 69 patients recovering from mild, moderate, severe, or critical COVID-19 in comparison to healthy uninfected controls. Twenty-one of these patients were referred to a long COVID clinic and > 50% reported ongoing symptoms more than 6 months post-infection.
Results: Anti-Spike and anti-RBD IgG responses were largely stable up to 24 wpi and correlated with disease severity. Deep immunophenotyping revealed significant differences in multiple innate (NK cells, LD neutrophils, CXCR3+ monocytes) and adaptive immune populations (T helper, T follicular helper, and regulatory T cells) in convalescent individuals compared to healthy controls, which were most strongly evident at 12 and 16 wpi. RNA sequencing revealed significant perturbations to gene expression in COVID-19 convalescents until at least 6 months post-infection. We also uncovered significant differences in the transcriptome at 24 wpi of convalescents who were referred to a long COVID clinic compared to those who were not.
Conclusions: Variation in the rate of recovery from infection at a cellular and transcriptional level may explain the persistence of symptoms associated with long COVID in some individuals.
Keywords: Antibody responses; COVID-19; Convalescent patients; Immunity; Immunophenotyping; Infection; Long COVID; Post COVID-19 condition; Post-acute sequelae of COVID-19 (PASC); RNA-Seq; SARS-CoV-2; T cell.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures





References
-
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Zhang L, Fan G, Xu J, Gu X, Cheng Z, Yu T, Xia J, Wei Y, Wu W, Xie X, Yin W, Li H, Liu M, Xiao Y, Gao H, Guo L, Xie J, Wang G, Jiang R, Gao Z, Jin Q, Wang J, Cao B. Clinical features of patients infected with 2019 novel coronavirus in Wuhan. China Lancet. 2020;395(10223):497–506. doi: 10.1016/S0140-6736(20)30183-5. - DOI - PMC - PubMed
-
- Huang C, Huang L, Wang Y, Li X, Ren L, Gu X, Kang L, Guo L, Liu M, Zhou X, Luo J, Huang Z, Tu S, Zhao Y, Chen L, Xu D, Li Y, Li C, Peng L, Li Y, Xie W, Cui D, Shang L, Fan G, Xu J, Wang G, Wang Y, Zhong J, Wang C, Wang J, Zhang D, Cao B. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet. 2021;397(10270):220–232. doi: 10.1016/S0140-6736(20)32656-8. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
