

Time-to-antibiotics and clinical outcomes in patients with sepsis and septic shock: a prospective nationwide multicenter cohort study
- PMID: 35027073
- PMCID: PMC8756674
- DOI: 10.1186/s13054-021-03883-0
Time-to-antibiotics and clinical outcomes in patients with sepsis and septic shock: a prospective nationwide multicenter cohort study
Abstract
Background: Timely administration of antibiotics is one of the most important interventions in reducing mortality in sepsis. However, administering antibiotics within a strict time threshold in all patients suspected with sepsis will require huge amount of effort and resources and may increase the risk of unintentional exposure to broad-spectrum antibiotics in patients without infection with its consequences. Thus, controversy still exists on whether clinicians should target different time-to-antibiotics thresholds for patients with sepsis versus septic shock.
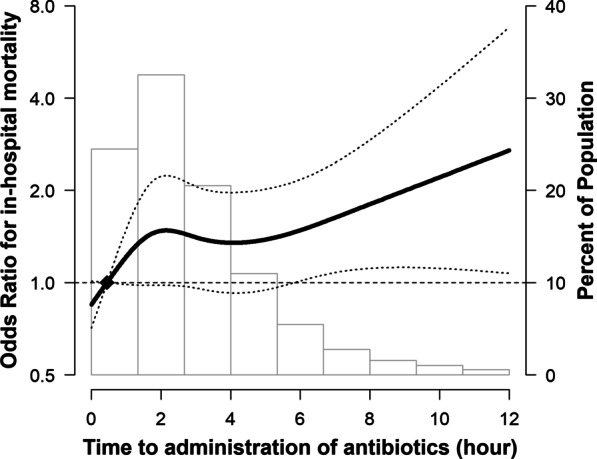
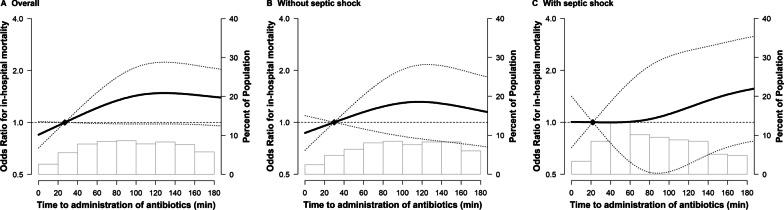
Methods: This study analyzed prospectively collected data from an ongoing multicenter cohort of patients with sepsis identified in the emergency department. Adjusted odds ratios (ORs) were compared for in-hospital mortality of patients who had received antibiotics within 1 h to that of those who did not. Spline regression models were used to assess the association of time-to-antibiotics as continuous variables and increasing risk of in-hospital mortality. The differences in the association between time-to-antibiotics and in-hospital mortality were assessed according to the presence of septic shock.
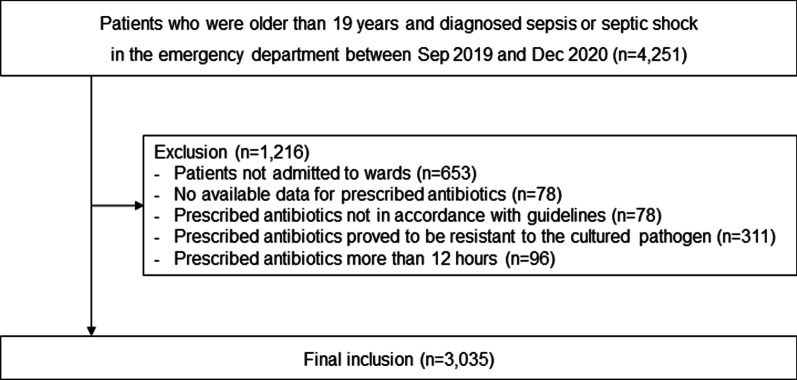
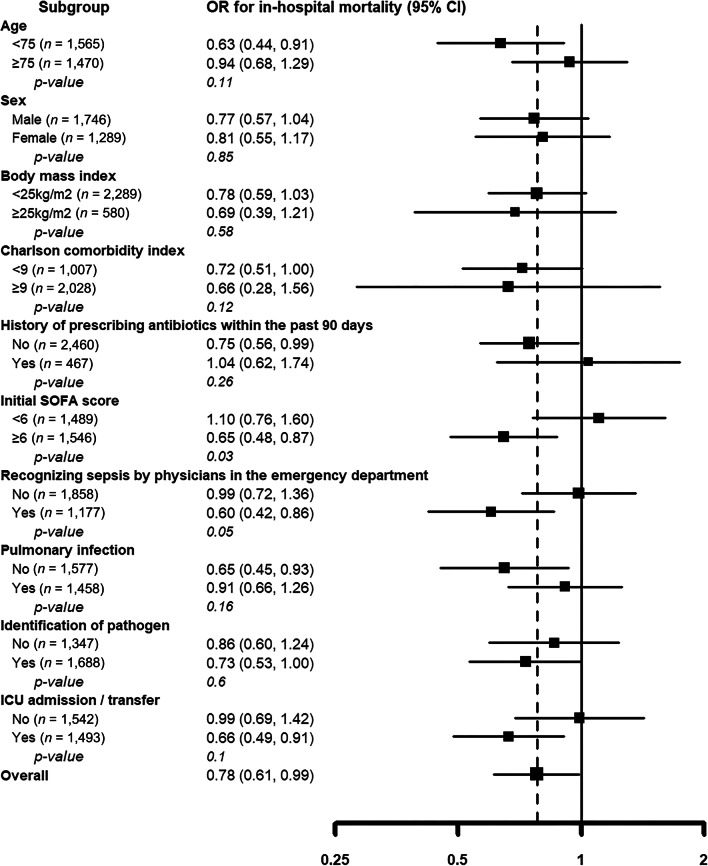
Results: Overall, 3035 patients were included in the analysis. Among them, 601 (19.8%) presented with septic shock, and 774 (25.5%) died. The adjusted OR for in-hospital mortality of patients whose time-to-antibiotics was within 1 h was 0.78 (95% confidence interval [CI] 0.61-0.99; p = 0.046). The adjusted OR for in-hospital mortality was 0.66 (95% CI 0.44-0.99; p = 0.049) and statistically significant in patients with septic shock, whereas it was 0.85 (95% CI 0.64-1.15; p = 0.300) in patients with sepsis but without shock. Among patients who received antibiotics within 3 h, those with septic shock showed 35% (p = 0.042) increased risk of mortality for every 1-h delay in antibiotics, but no such trend was observed in patients without shock.
Conclusion: Timely administration of antibiotics improved outcomes in patients with septic shock; however, the association between early antibiotic administration and outcome was not as clear in patients with sepsis without shock.
Keywords: Hour-1 bundle; Mortality; Sepsis; Septic shock; Time-to-antibiotics.
© 2022. The Author(s).
Conflict of interest statement
All authors declare that they have no competing interests.
Figures
References
-
- Ferrer R, Martin-Loeches I, Phillips G, Osborn TM, Townsend S, Dellinger RP, et al. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: results from a guideline-based performance improvement program. Crit Care Med. 2014;42(8):1749–1755. doi: 10.1097/CCM.0000000000000330. - DOI - PubMed
-
- Kumar A, Roberts D, Wood KE, Light B, Parrillo JE, Sharma S, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med. 2006;34(6):1589–1596. doi: 10.1097/01.CCM.0000217961.75225.E9. - DOI - PubMed
-
- Gaieski DF, Mikkelsen ME, Band RA, Pines JM, Massone R, Furia FF, et al. Impact of time to antibiotics on survival in patients with severe sepsis or septic shock in whom early goal-directed therapy was initiated in the emergency department. Crit Care Med. 2010;38(4):1045–1053. doi: 10.1097/CCM.0b013e3181cc4824. - DOI - PubMed
-
- Garnacho-Montero J, Aldabo-Pallas T, Garnacho-Montero C, Cayuela A, Jiménez R, Barroso S, et al. Timing of adequate antibiotic therapy is a greater determinant of outcome than are TNF and IL-10 polymorphisms in patients with sepsis. Crit Care. 2006;10(4):R111. doi: 10.1186/cc4995. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
