

Fluorescent Molecular Imaging Can Improve Intraoperative Sentinel Margin Detection in Oral Squamous Cell Carcinoma
- PMID: 35027369
- PMCID: PMC9364343
- DOI: 10.2967/jnumed.121.262235
Fluorescent Molecular Imaging Can Improve Intraoperative Sentinel Margin Detection in Oral Squamous Cell Carcinoma
Abstract
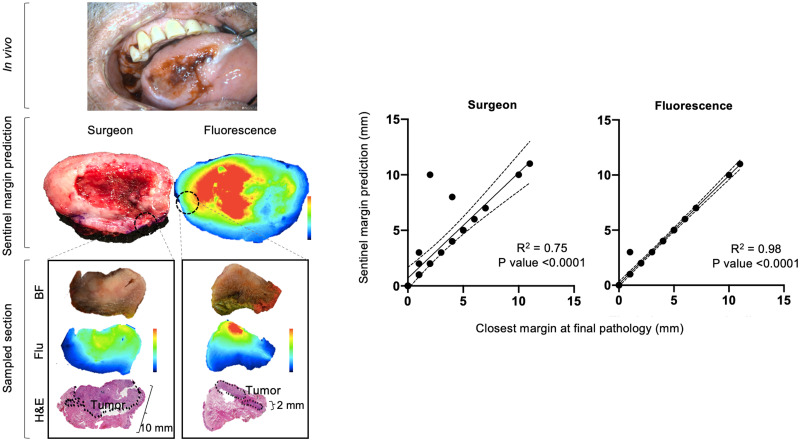
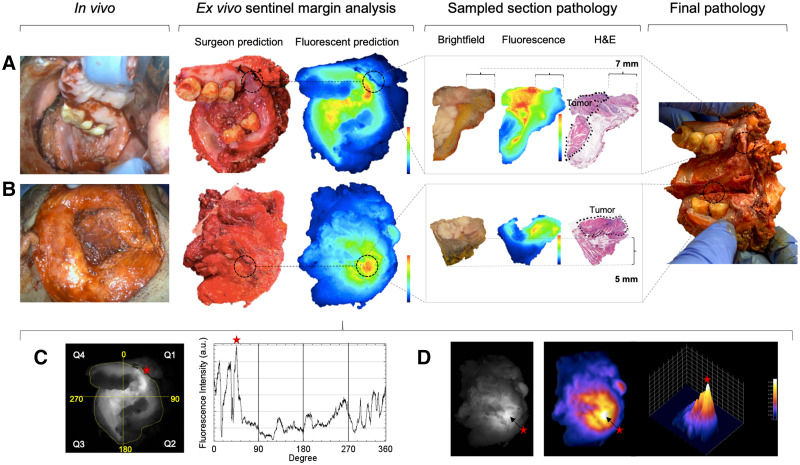
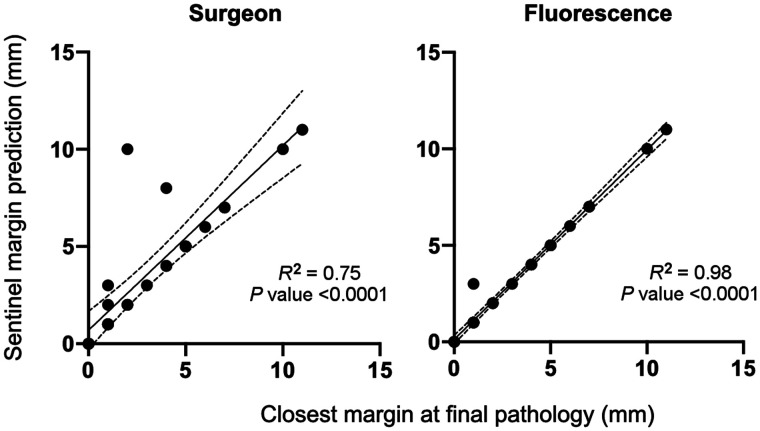
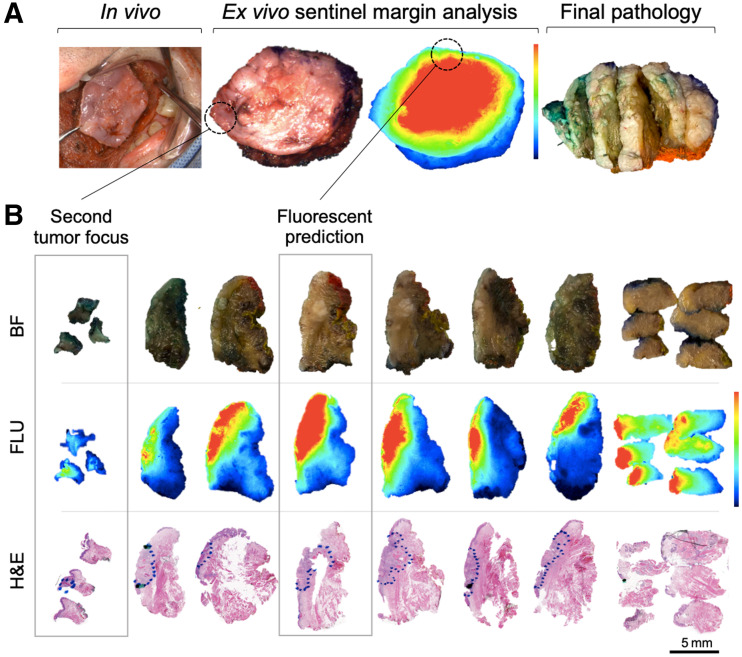
In head and neck cancer, a major limitation of current intraoperative margin analysis is the ability to detect areas most likely to be positive based on specimen palpation, especially for larger specimens where sampling error limits detection of positive margins. This study aims to prospectively examine the clinical value of fluorescent molecular imaging to accurately identify "the sentinel margin," the point on a specimen at which the tumor lies closest to the resected edge in real-time during frozen section analysis. Methods: Eighteen patients with oral squamous cell carcinoma were enrolled into a prospective clinical trial and infused intravenously with 50 mg of panitumumab-IRDye800CW 1-5 d before surgery. Resected specimens were imaged in a closed-field near-infrared optical imaging system in near real-time, and custom-designed software was used to identify locations of highest fluorescence on deep and peripheral margins. The surgeon identified the sentinel margin masked to optical specimen mapping, and then the regions of highest fluorescence were identified and marked for frozen analysis. Final pathology based on specimen reconstruction was used as reference standard. Results: Resected specimens were imaged in the operating room, and fluorescence had a higher interobserver agreement with pathology (Cohen κ value 0.96) than the surgeon (Cohen κ value of 0.82) for the location of the closest margin. Plotting margin distance at the predicted sentinel margin location of each observer versus the actual closest margin distance at pathology demonstrated best correlation between fluorescence and pathology (R2 = 0.98) with surgeon (R2 = 0.75). Conclusion: Fluorescence imaging can improve identification of the sentinel margin in head and neck cancer resections, holding promise for rapid identification of positive margins and improved oncologic outcomes.
Keywords: fluorescent image-guided surgery; head and neck cancer; oral squamous cell carcinoma; surgical oncology; tumor margins.
© 2022 by the Society of Nuclear Medicine and Molecular Imaging.
Figures
Similar articles
-
The Sentinel Margin: Intraoperative Ex Vivo Specimen Mapping Using Relative Fluorescence Intensity.Clin Cancer Res. 2019 Aug 1;25(15):4656-4662. doi: 10.1158/1078-0432.CCR-19-0319. Epub 2019 May 29. Clin Cancer Res. 2019. PMID: 31142505 Free PMC article. Clinical Trial.
-
Intraoperative Molecular Imaging for ex vivo Assessment of Peripheral Margins in Oral Squamous Cell Carcinoma.Front Oncol. 2020 Jan 10;9:1476. doi: 10.3389/fonc.2019.01476. eCollection 2019. Front Oncol. 2020. PMID: 31998640 Free PMC article.
-
Improved intraoperative identification of close margins in oral squamous cell carcinoma resections using a dual aperture fluorescence ratio approach: first in-human results.J Biomed Opt. 2024 Jan;29(1):016003. doi: 10.1117/1.JBO.29.1.016003. Epub 2024 Jan 17. J Biomed Opt. 2024. PMID: 38235321 Free PMC article.
-
Intraoperative Fluorescence-Guided Surgery in Head and Neck Squamous Cell Carcinoma.Laryngoscope. 2021 Mar;131(3):529-534. doi: 10.1002/lary.28822. Epub 2020 Jul 3. Laryngoscope. 2021. PMID: 33593036 Review.
-
Improving oral cavity cancer diagnosis and treatment with fluorescence molecular imaging.Oral Dis. 2021 Jan;27(1):21-26. doi: 10.1111/odi.13308. Epub 2020 Mar 13. Oral Dis. 2021. PMID: 32072691 Free PMC article. Review.
Cited by
-
Cutting-edge insights: near-infrared imaging for surgical margin assessment in head and neck tumor resection: a systematic review and meta-analysis.Quant Imaging Med Surg. 2024 Dec 5;14(12):8167-8182. doi: 10.21037/qims-24-564. Epub 2024 Nov 8. Quant Imaging Med Surg. 2024. PMID: 39698655 Free PMC article.
-
Interim Phase II Results Using Panitumumab-IRDye800CW during Transoral Robotic Surgery in Patients with Oropharyngeal Cancer.Clin Cancer Res. 2024 Sep 13;30(18):4016-4028. doi: 10.1158/1078-0432.CCR-24-0940. Clin Cancer Res. 2024. PMID: 39012279 Free PMC article. Clinical Trial.
-
Fluorescence Imaging-Assessed Surgical Margin Detection in Head and Neck Oncology by Passive and Active Targeting.Mol Diagn Ther. 2025 Jul;29(4):465-481. doi: 10.1007/s40291-025-00781-x. Epub 2025 May 8. Mol Diagn Ther. 2025. PMID: 40342044 Free PMC article. Review.
-
Identification of Optimal Tissue-Marking Dye Color for Pathological Evaluation in Fluorescence Imaging Using IRDye800CW.Mol Imaging Biol. 2024 Feb;26(1):162-172. doi: 10.1007/s11307-023-01882-x. Epub 2023 Dec 6. Mol Imaging Biol. 2024. PMID: 38057647
-
Optical molecular imaging in oral- and oropharyngeal squamous cell carcinoma using a novel uPAR-targeting near-infrared imaging agent FG001 (ICG-Glu-Glu-AE105): An explorative phase II clinical trial.Theranostics. 2025 Jan 1;15(1):52-67. doi: 10.7150/thno.100042. eCollection 2025. Theranostics. 2025. PMID: 39744227 Free PMC article. Clinical Trial.
References
-
- Luryi AL, Chen MM, Mehra S, Roman SA, Sosa JA, Judson BL. Positive surgical margins in early stage oral cavity cancer: an analysis of 20,602 cases. Otolaryngol Head Neck Surg. 2014;151:984–990. - PubMed
-
- Smits RW, Koljenović S, Hardillo JA, et al. . Resection margins in oral cancer surgery: Room for improvement. Head Neck. 2016;38(suppl 1):E2197–E2203. - PubMed
-
- Kain JJ, Birkeland AC, Udayakumar N, et al. . Surgical margins in oral cavity squamous cell carcinoma: current practices and future directions. Laryngoscope. 2020;130:128–138. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical