Current and novel biomarkers of thrombotic risk in COVID-19: a Consensus Statement from the International COVID-19 Thrombosis Biomarkers Colloquium
- PMID: 35027697
- PMCID: PMC8757397
- DOI: 10.1038/s41569-021-00665-7
Current and novel biomarkers of thrombotic risk in COVID-19: a Consensus Statement from the International COVID-19 Thrombosis Biomarkers Colloquium
Abstract
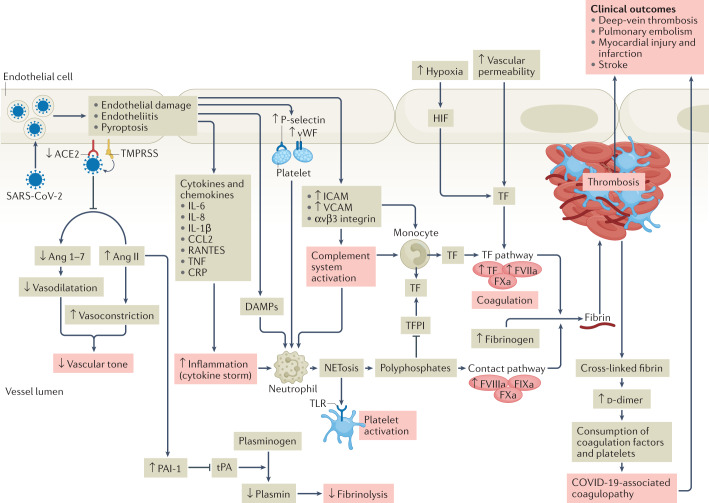
Coronavirus disease 2019 (COVID-19) predisposes patients to thrombotic and thromboembolic events, owing to excessive inflammation, endothelial cell activation and injury, platelet activation and hypercoagulability. Patients with COVID-19 have a prothrombotic or thrombophilic state, with elevations in the levels of several biomarkers of thrombosis, which are associated with disease severity and prognosis. Although some biomarkers of COVID-19-associated coagulopathy, including high levels of fibrinogen and D-dimer, were recognized early during the pandemic, many new biomarkers of thrombotic risk in COVID-19 have emerged. In this Consensus Statement, we delineate the thrombotic signature of COVID-19 and present the latest biomarkers and platforms to assess the risk of thrombosis in these patients, including markers of platelet activation, platelet aggregation, endothelial cell activation or injury, coagulation and fibrinolysis as well as biomarkers of the newly recognized post-vaccine thrombosis with thrombocytopenia syndrome. We then make consensus recommendations for the clinical use of these biomarkers to inform prognosis, assess disease acuity, and predict thrombotic risk and in-hospital mortality. A thorough understanding of these biomarkers might aid risk stratification and prognostication, guide interventions and provide a platform for future research.
© 2022. Springer Nature Limited.
Conflict of interest statement
P.A.G. has received consulting fees and/or honoraria from Bayer, Hikari Dx, Janssen, Medicure, Otitopic, UpToDate and US WorldMeds, and institutional research grants from Amgen, Bayer, Haemonetics, Idorsia, Instrumentation Laboratories, Janssen, the NIH, Medicure, Otitopic and US WorldMeds. H.t.C. is a shareholder of Coagulation Profile and a consultant for Alveron. R.C.B. is a scientific advisor for Basking Biosciences. The other authors declare no competing interests.
Figures