

T cell characteristics associated with toxicity to immune checkpoint blockade in patients with melanoma
- PMID: 35027754
- PMCID: PMC8866214
- DOI: 10.1038/s41591-021-01623-z
T cell characteristics associated with toxicity to immune checkpoint blockade in patients with melanoma
Abstract
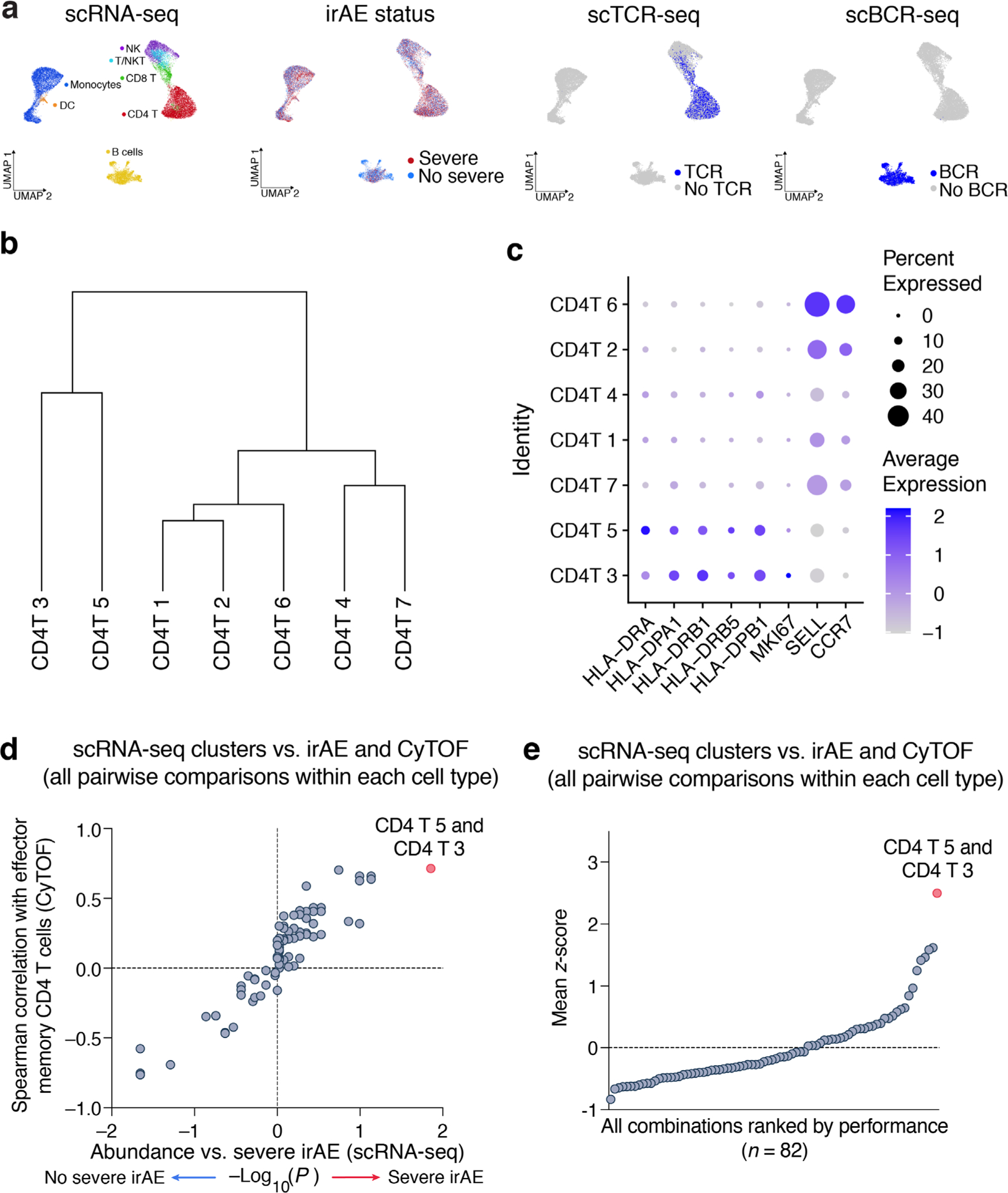
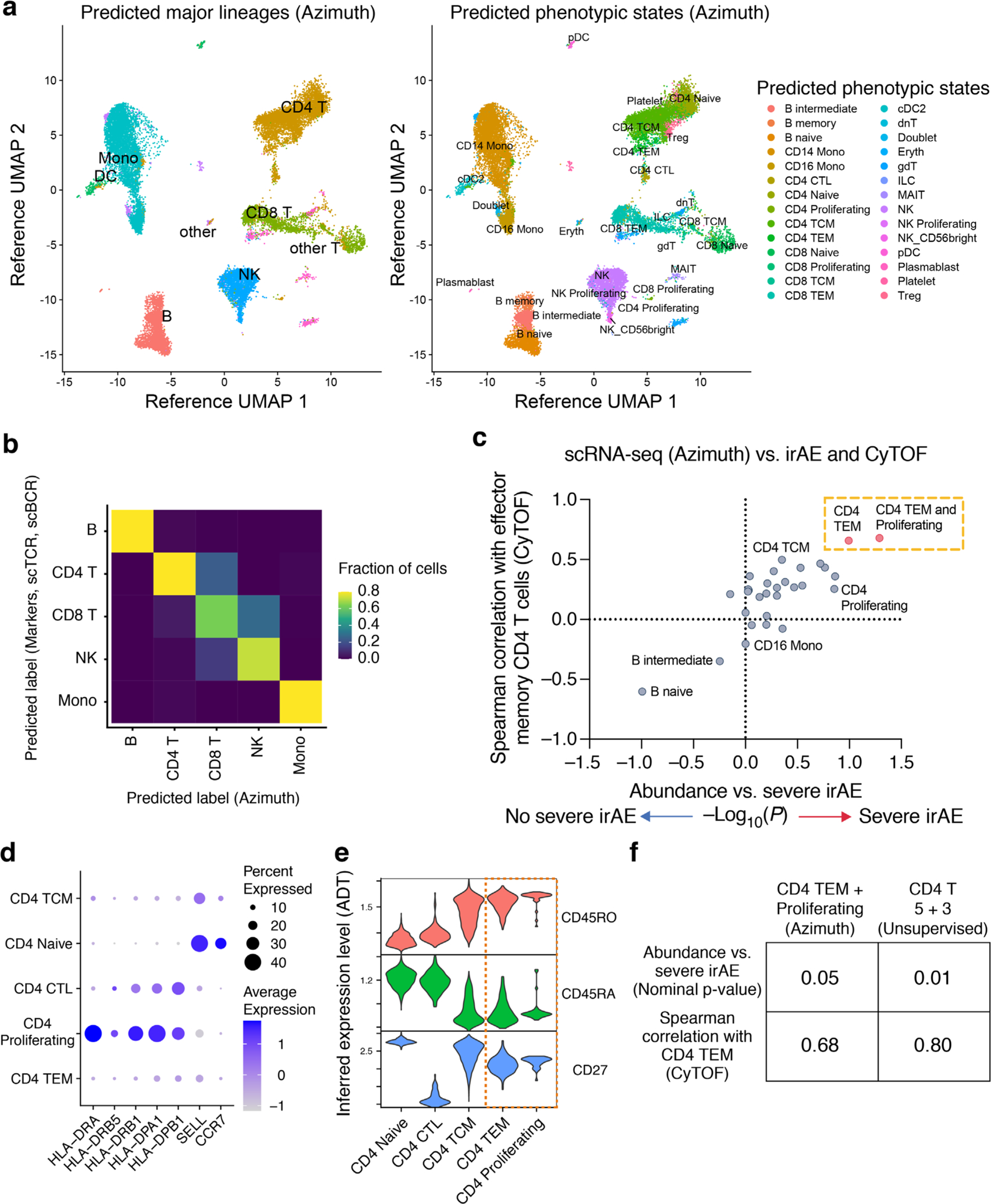
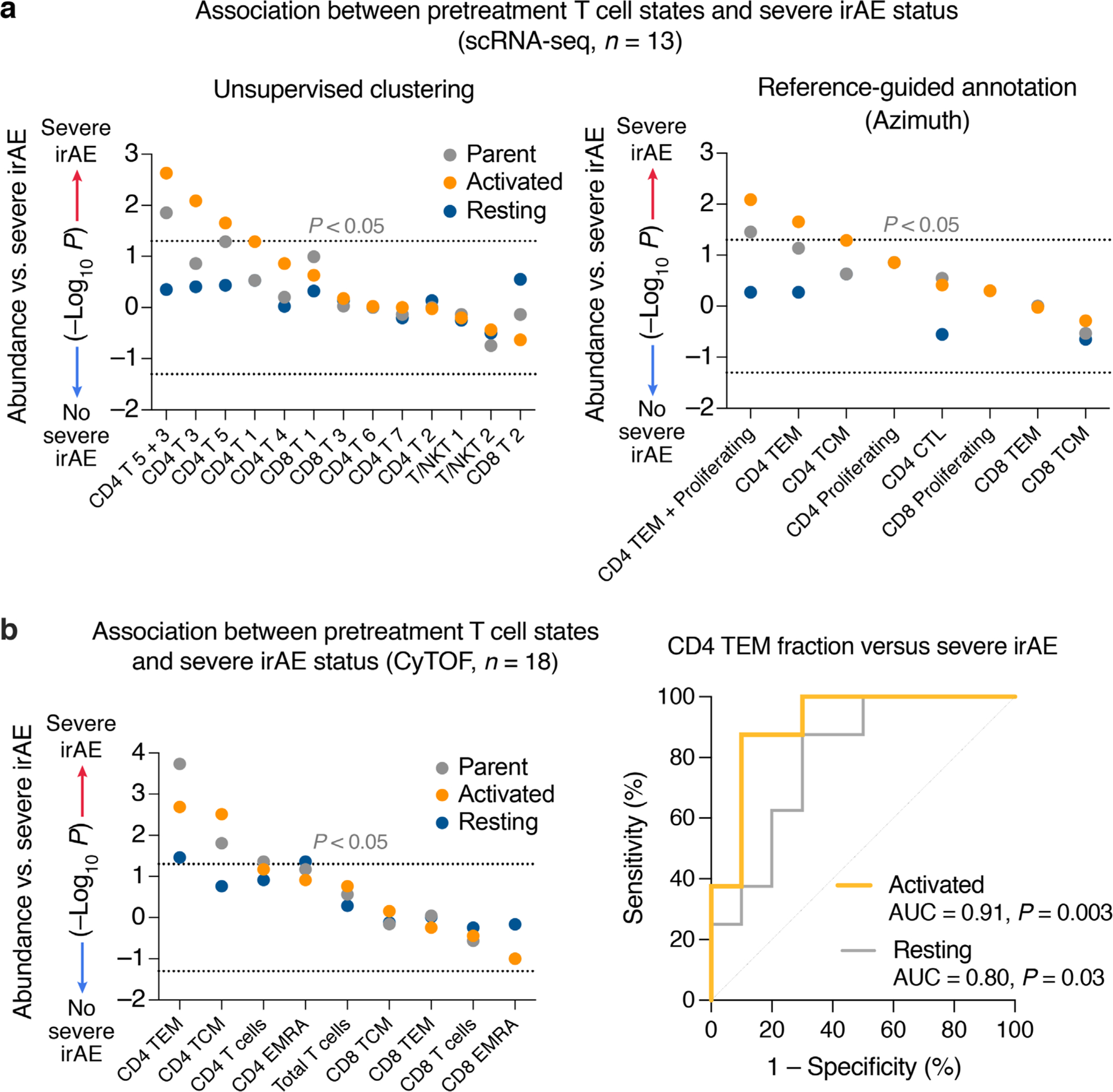
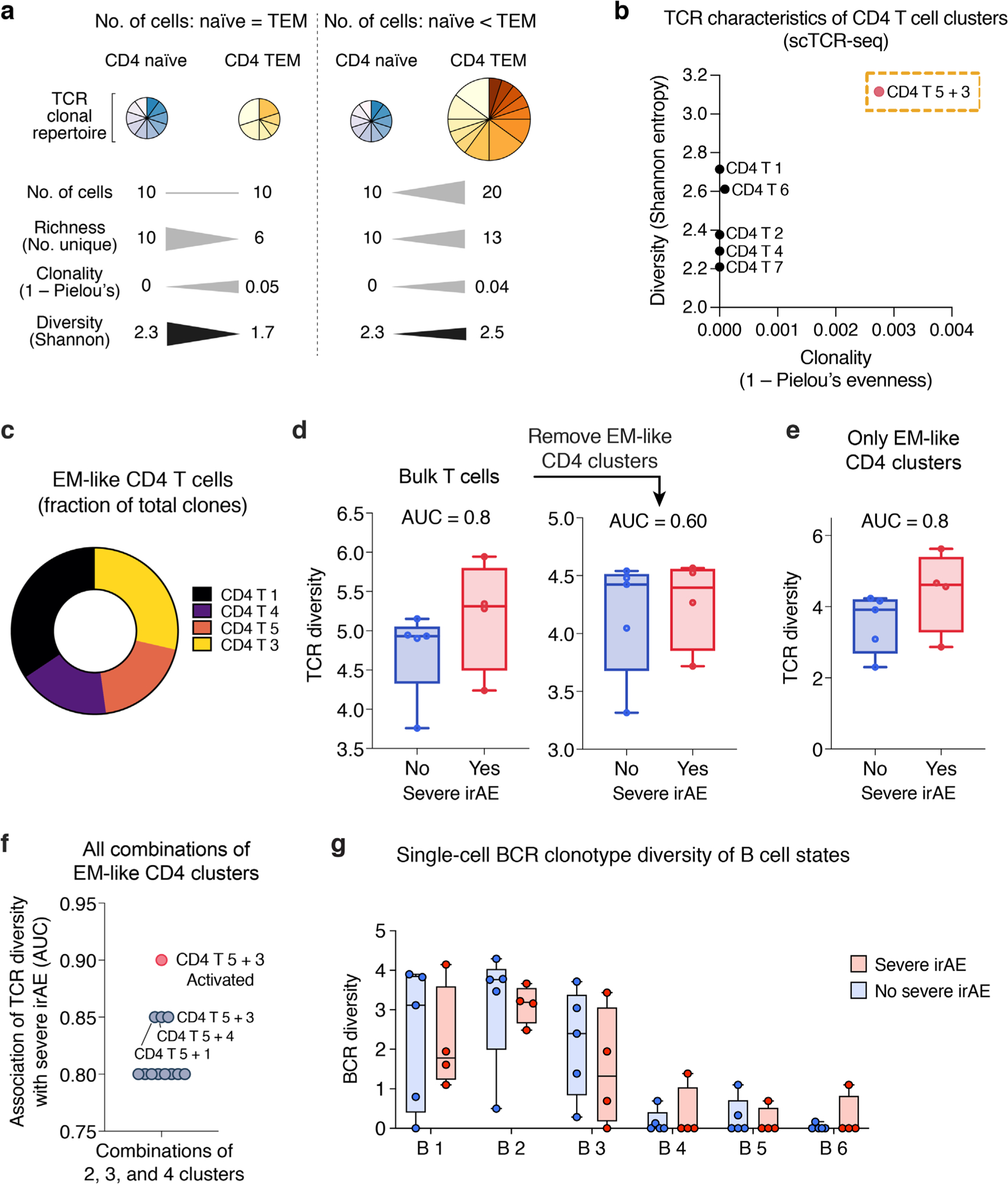
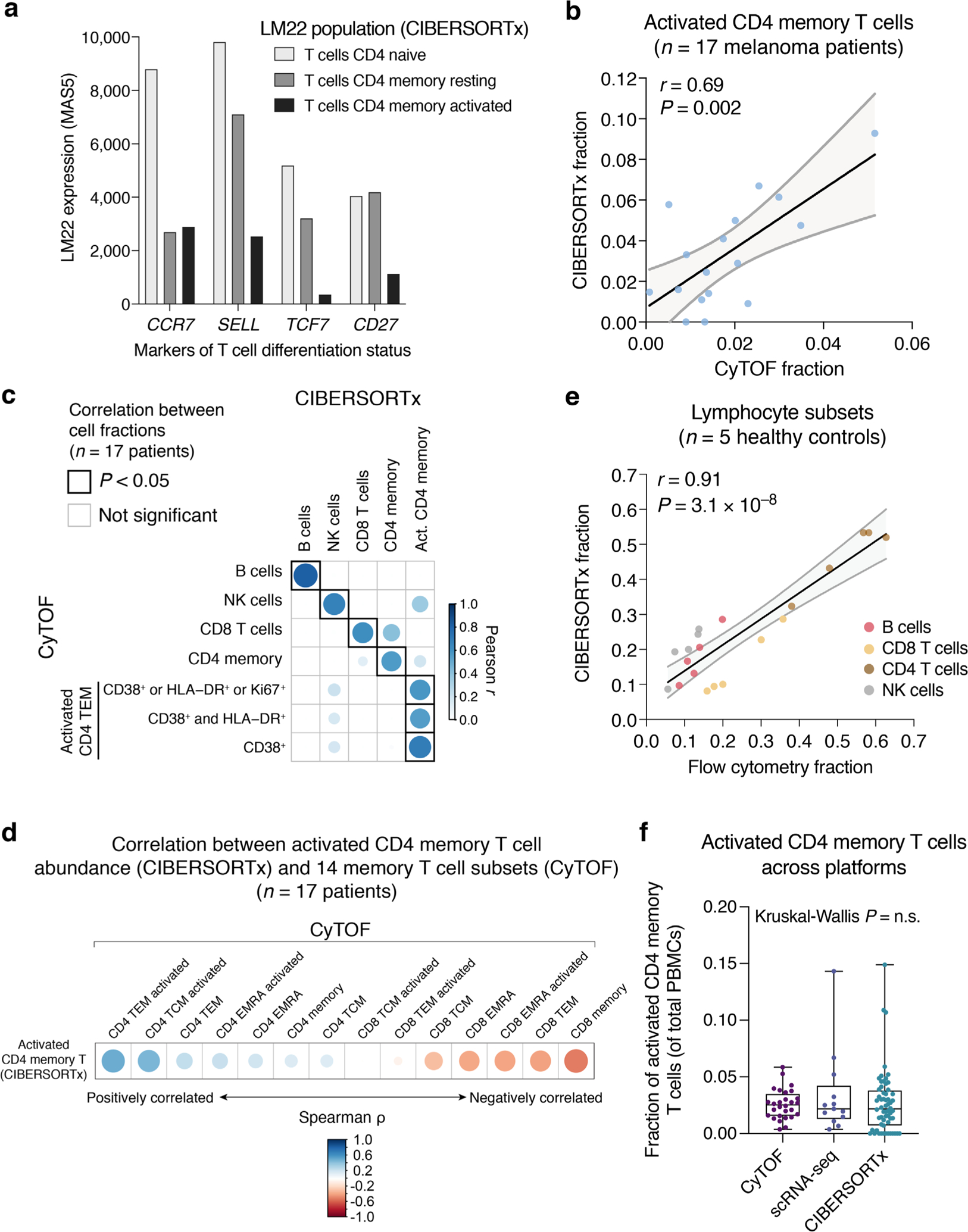
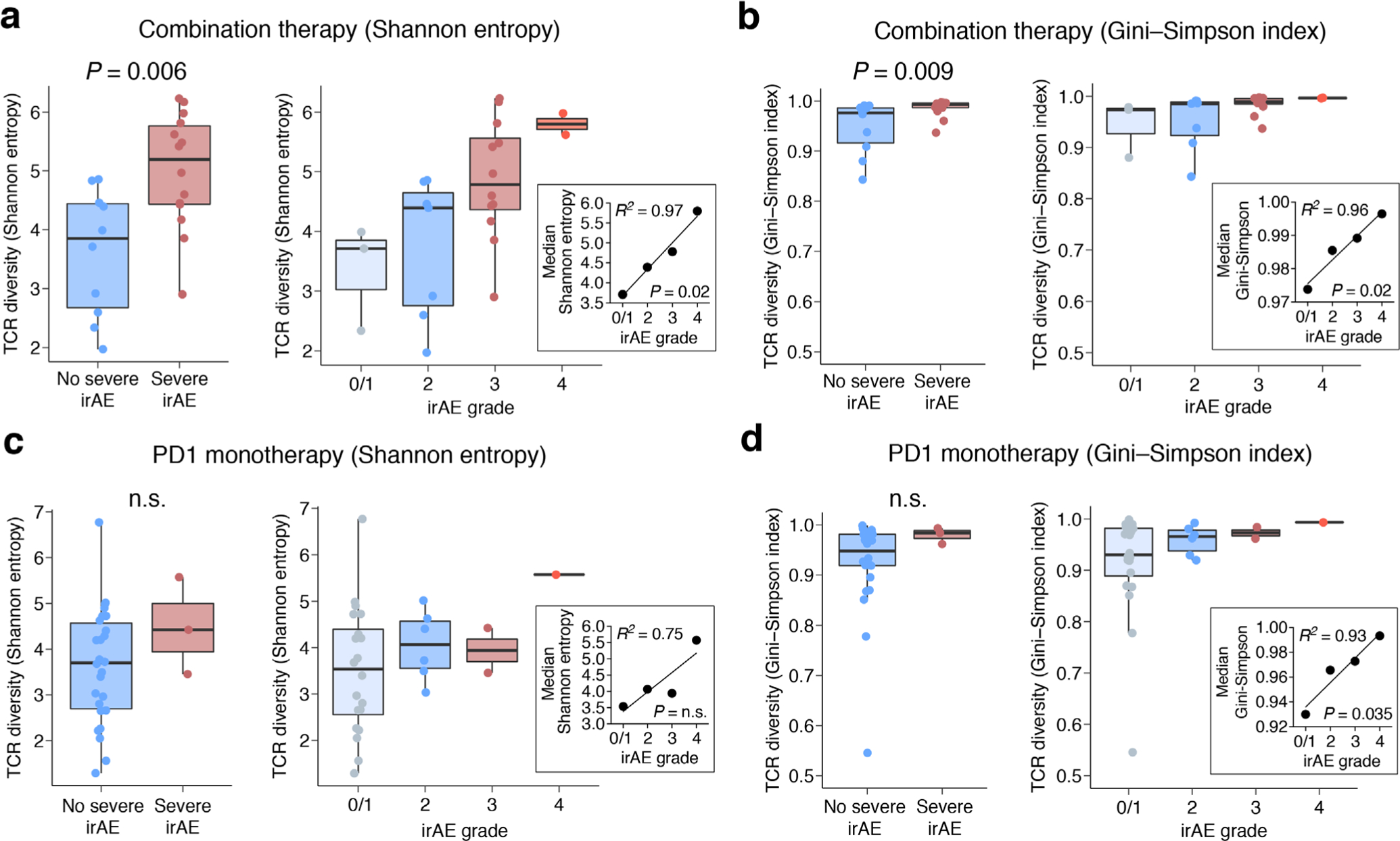
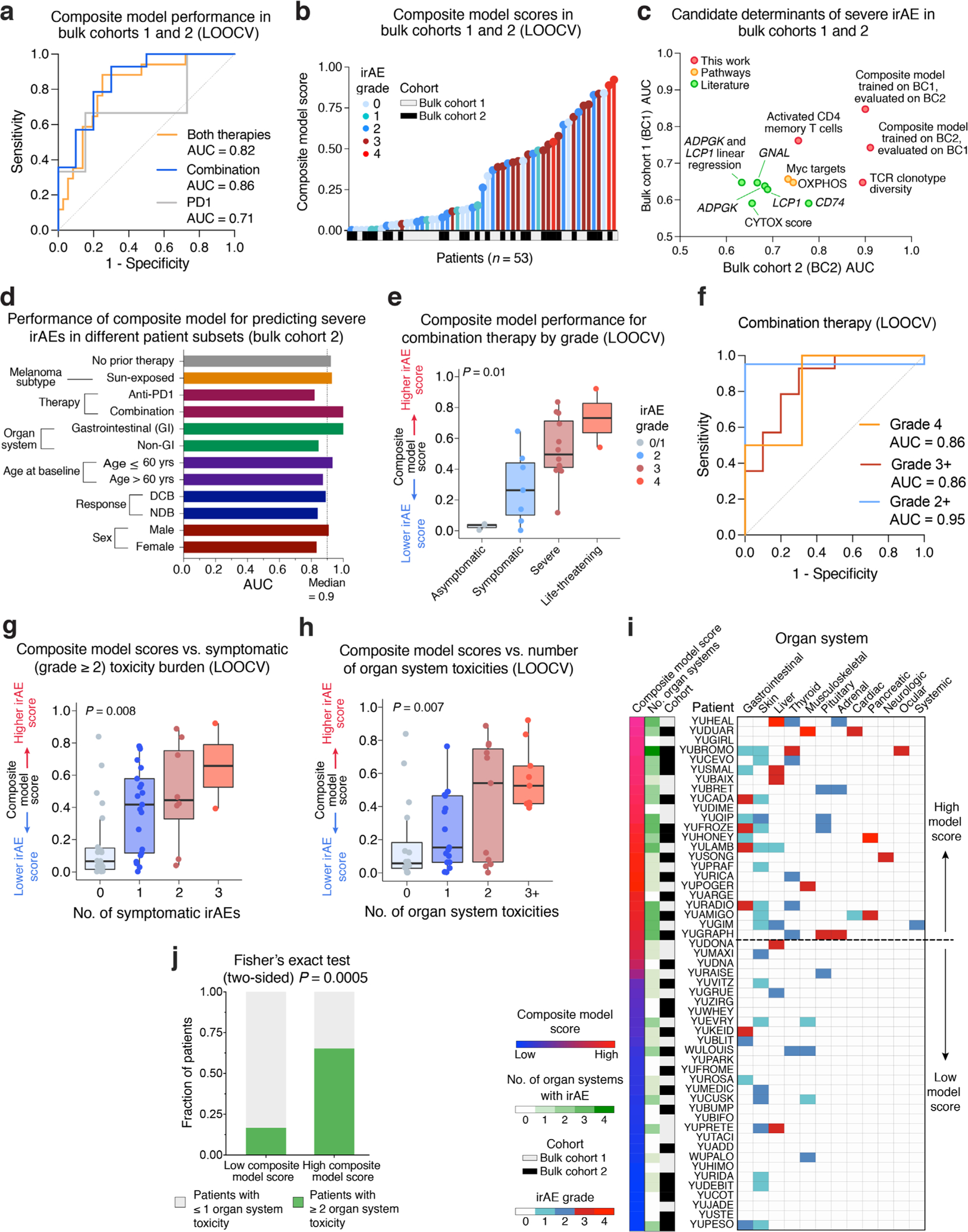
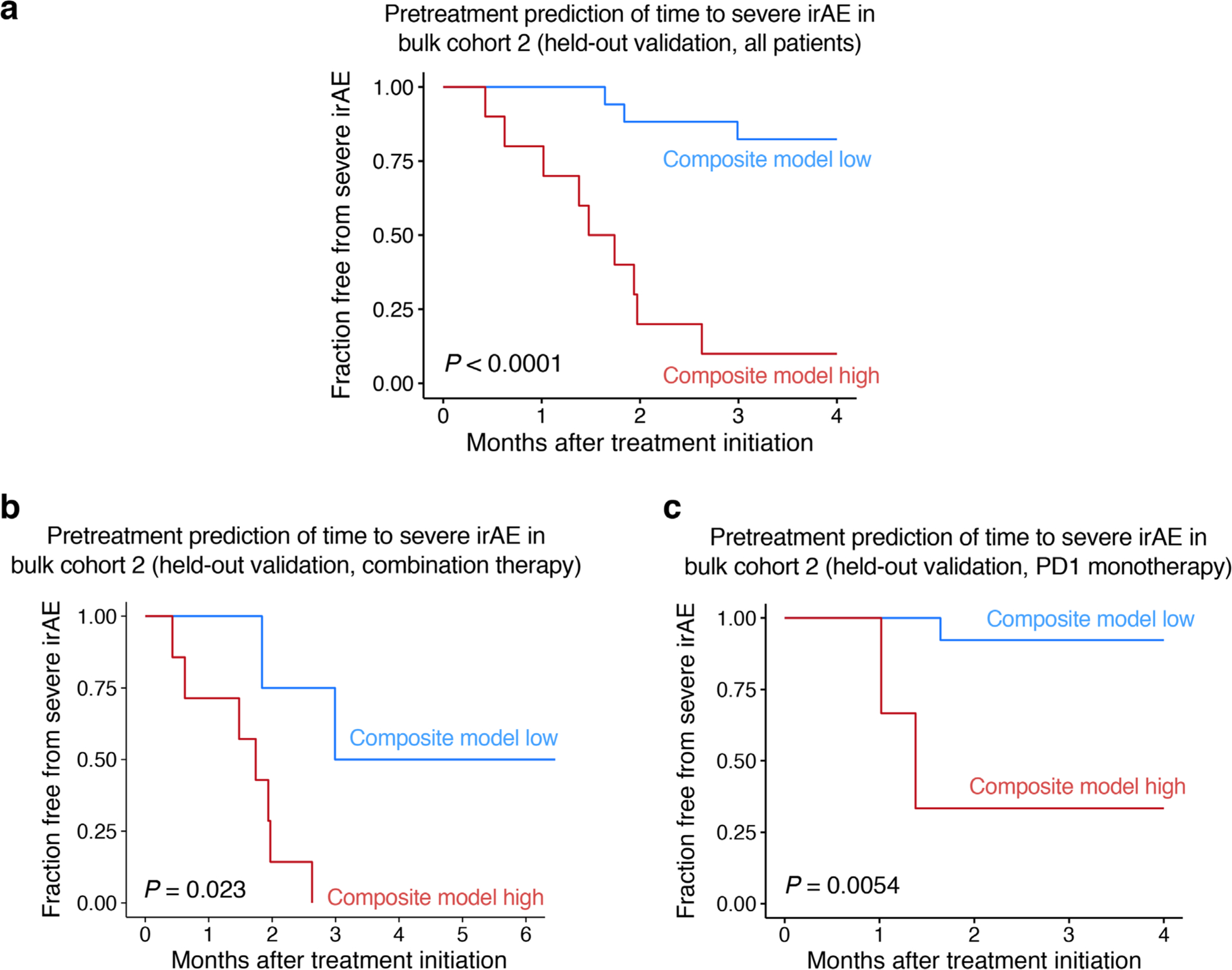
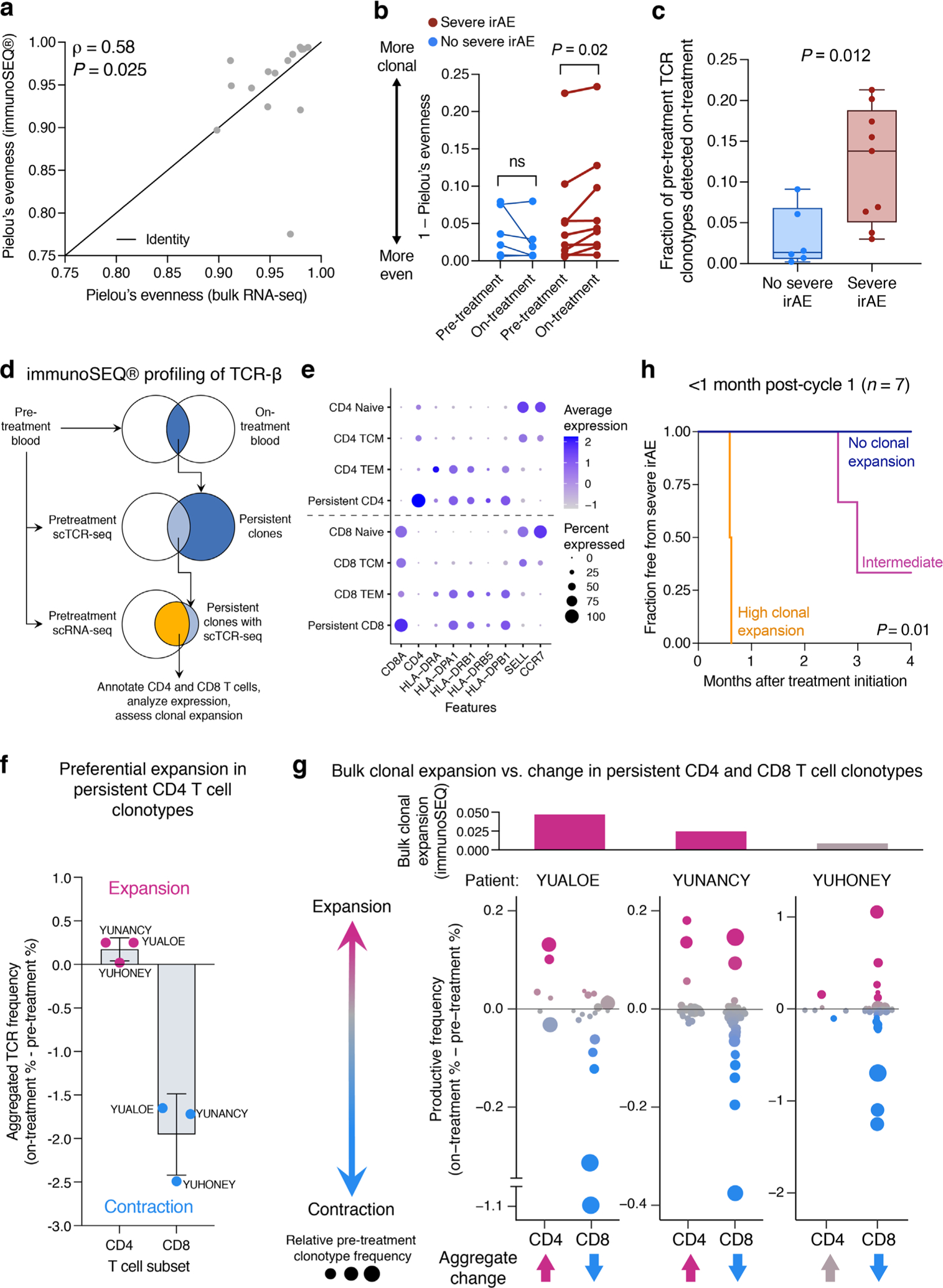
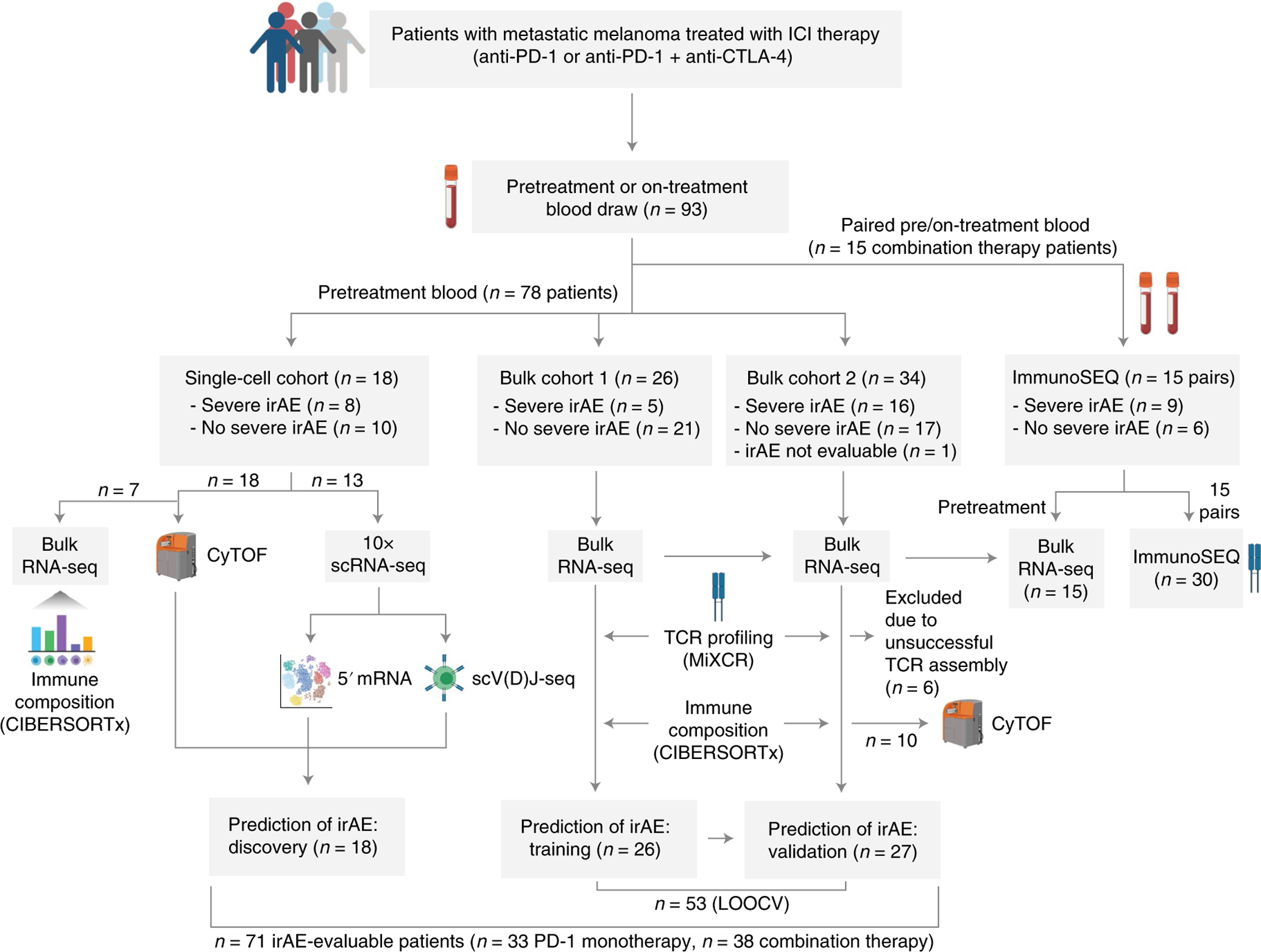
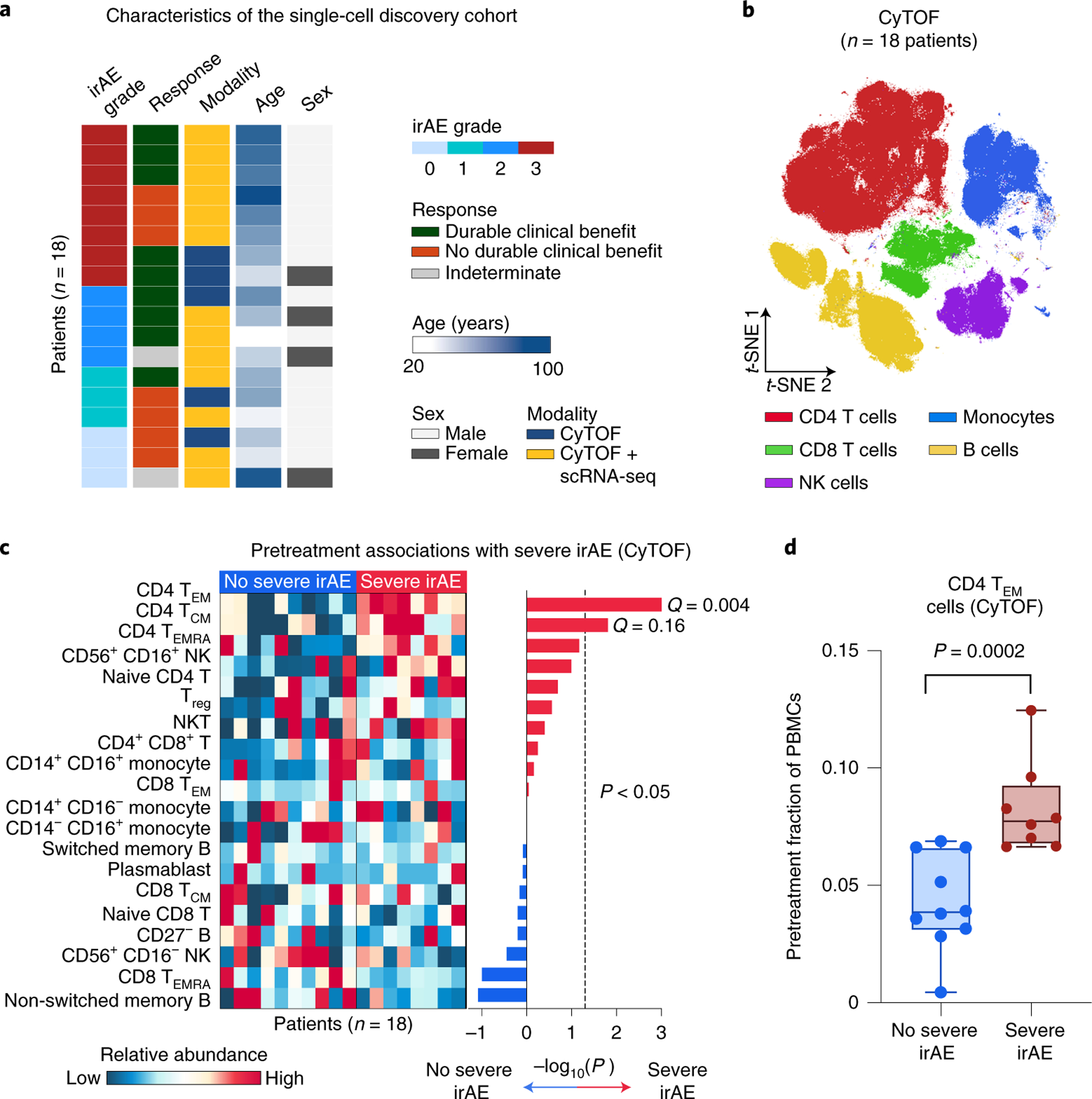
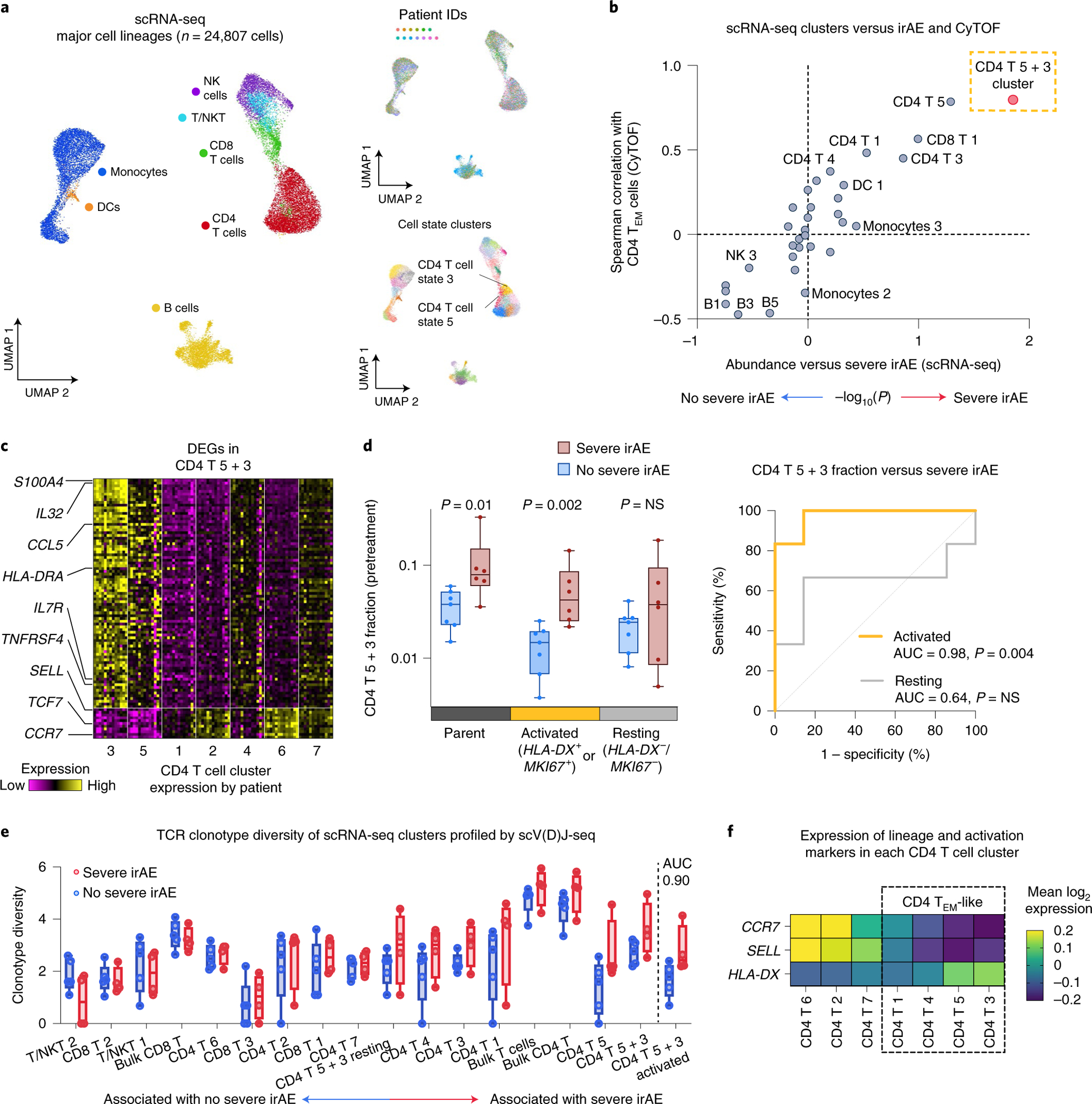
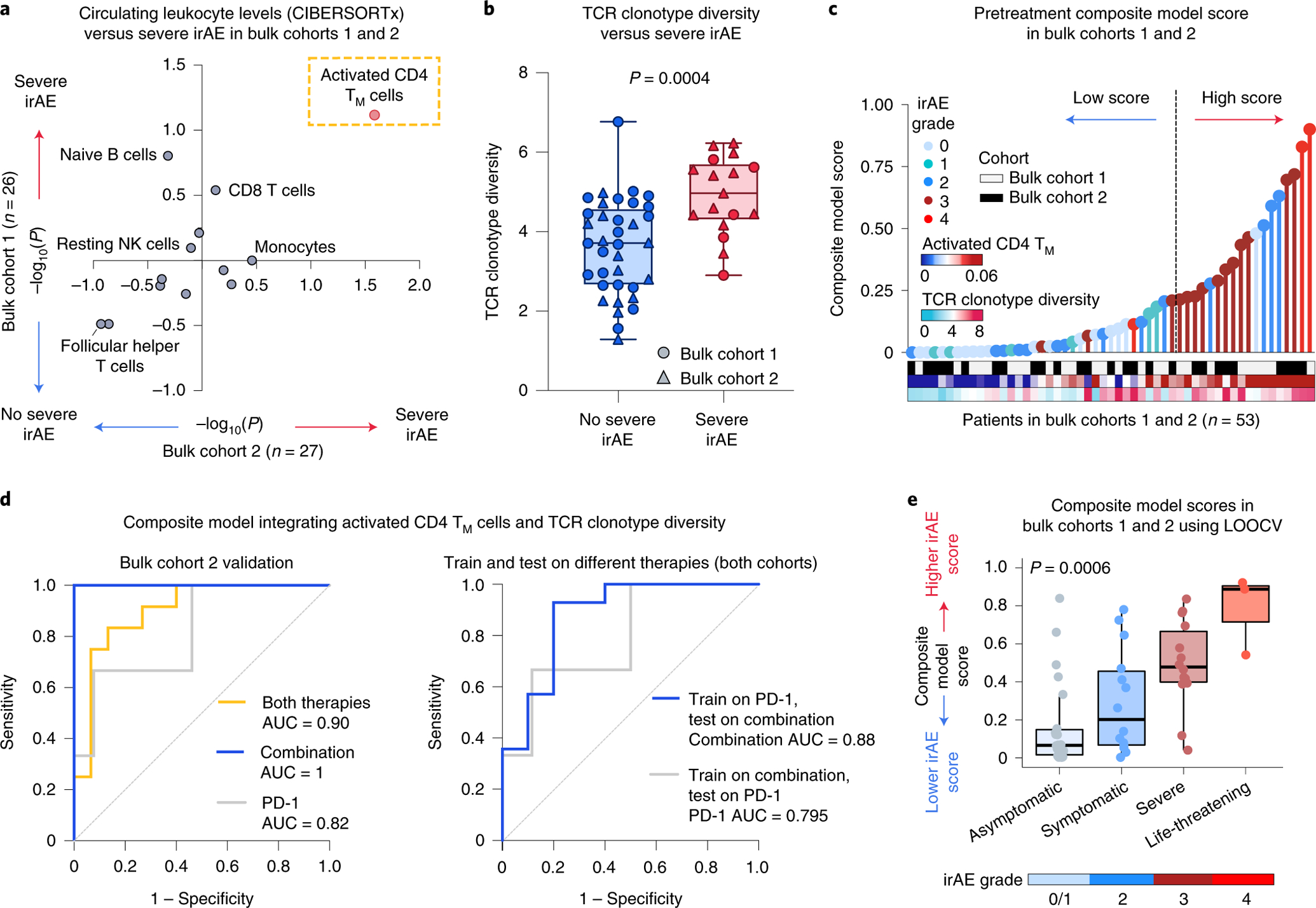
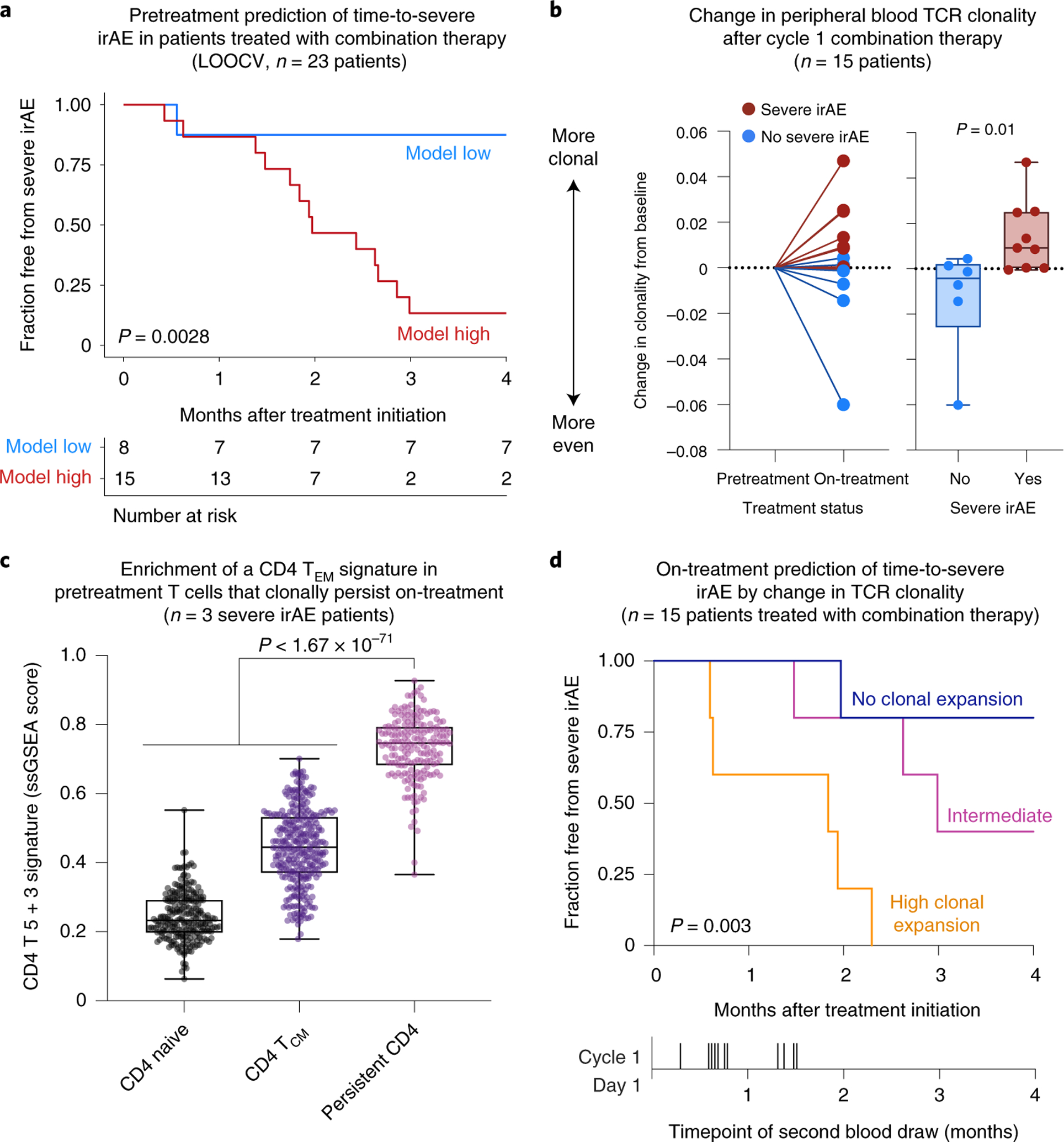
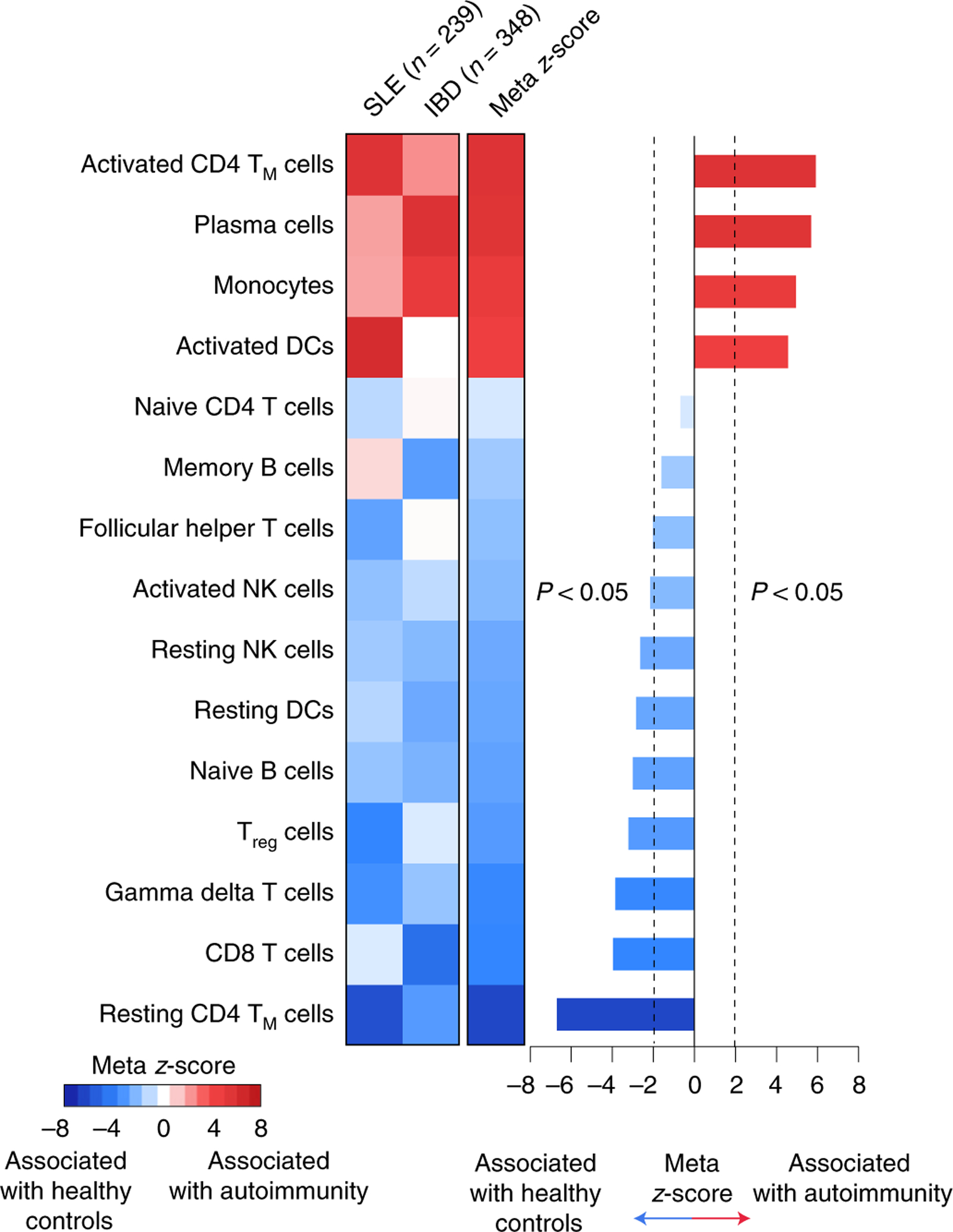
Severe immune-related adverse events (irAEs) occur in up to 60% of patients with melanoma treated with immune checkpoint inhibitors (ICIs). However, it is unknown whether a common baseline immunological state precedes irAE development. Here we applied mass cytometry by time of flight, single-cell RNA sequencing, single-cell V(D)J sequencing, bulk RNA sequencing and bulk T cell receptor (TCR) sequencing to study peripheral blood samples from patients with melanoma treated with anti-PD-1 monotherapy or anti-PD-1 and anti-CTLA-4 combination ICIs. By analyzing 93 pre- and early on-ICI blood samples and 3 patient cohorts (n = 27, 26 and 18), we found that 2 pretreatment factors in circulation-activated CD4 memory T cell abundance and TCR diversity-are associated with severe irAE development regardless of organ system involvement. We also explored on-treatment changes in TCR clonality among patients receiving combination therapy and linked our findings to the severity and timing of irAE onset. These results demonstrate circulating T cell characteristics associated with ICI-induced toxicity, with implications for improved diagnostics and clinical management.
© 2022. The Author(s), under exclusive licence to Springer Nature America, Inc.
Figures
Comment in
-
Elevated circulating memory T cells precede immunotherapy toxicities in melanoma.Trends Cancer. 2022 May;8(5):347-349. doi: 10.1016/j.trecan.2022.02.008. Epub 2022 Mar 8. Trends Cancer. 2022. PMID: 35277376
-
Primed for toxicity: CD4+ T cells and immune checkpoint inhibitors.Med. 2022 Mar 11;3(3):155-156. doi: 10.1016/j.medj.2022.02.003. Med. 2022. PMID: 35590189
References
-
- Hodi FS et al. Nivolumab plus ipilimumab or nivolumab alone versus ipilimumab alone in advanced melanoma (CheckMate 067): 4-year outcomes of a multicentre, randomised, phase 3 trial. Lancet Oncol 19, 1480–1492 (2018). - PubMed
-
- Postow MA, Sidlow R & Hellmann MD Immune-related adverse events associated with immune checkpoint blockade. N. Engl. J. Med 378, 158–168 (2018). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
