

SARS-CoV-2 infection and COVID-19 vaccination rates in pregnant women in Scotland
- PMID: 35027756
- PMCID: PMC8938271
- DOI: 10.1038/s41591-021-01666-2
SARS-CoV-2 infection and COVID-19 vaccination rates in pregnant women in Scotland
Erratum in
-
Author Correction: SARS-CoV-2 infection and COVID-19 vaccination rates in pregnant women in Scotland.Nat Med. 2022 Mar;28(3):599. doi: 10.1038/s41591-022-01730-5. Nat Med. 2022. PMID: 35121824 Free PMC article. No abstract available.
Abstract
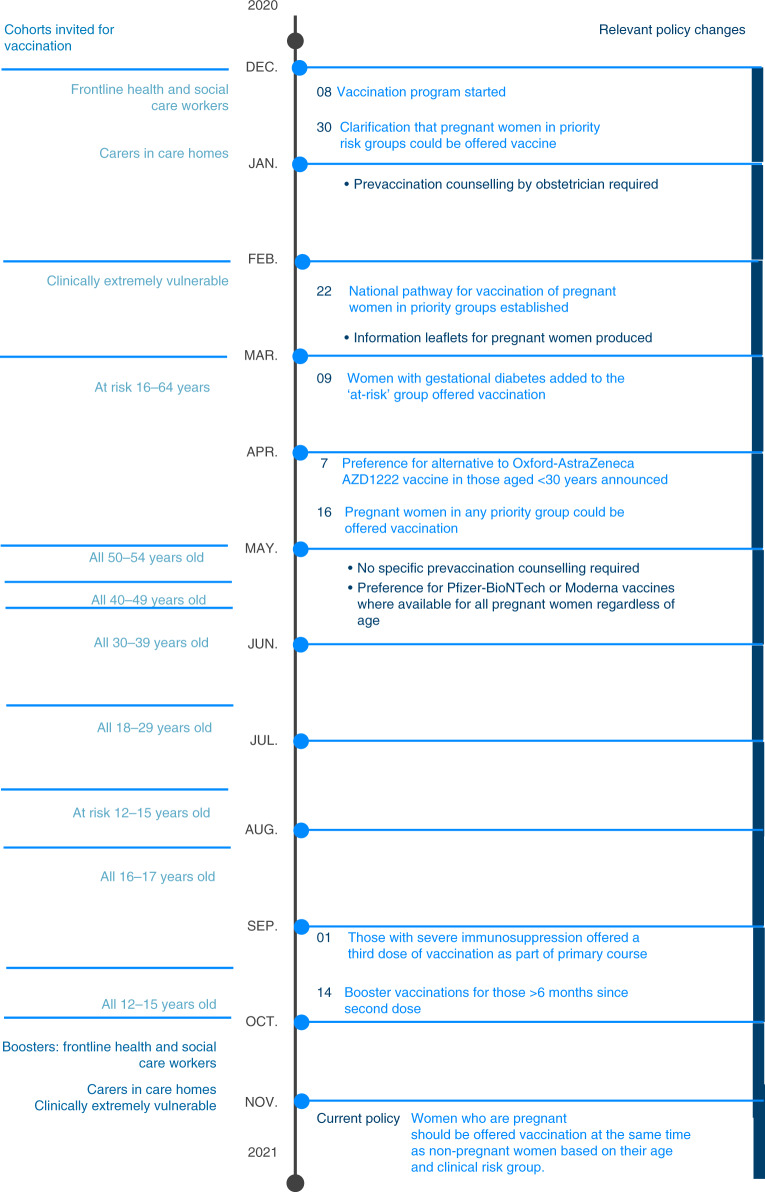
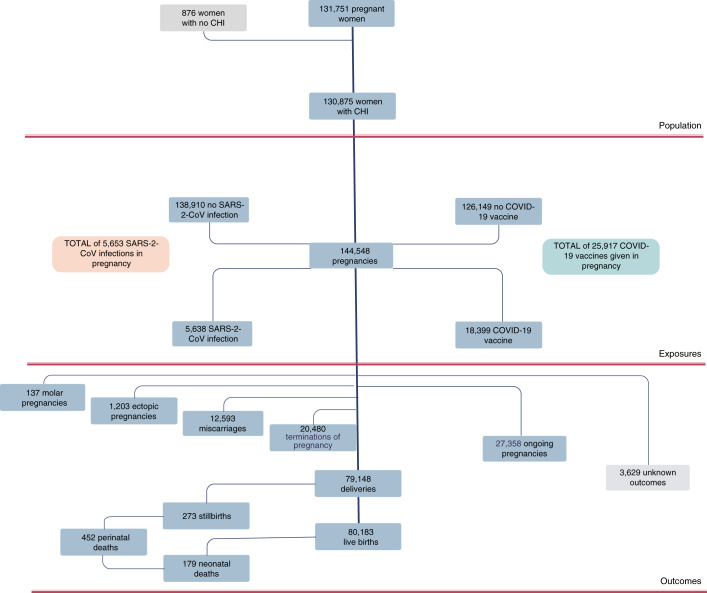
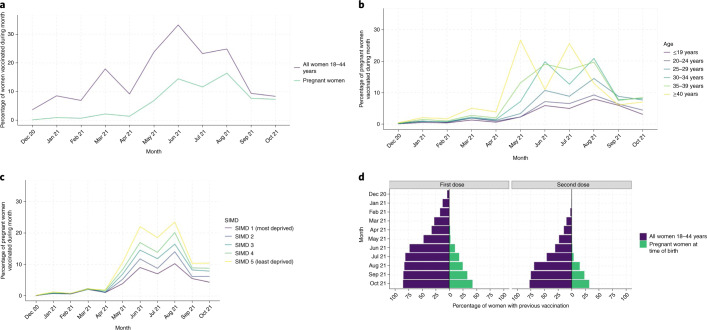
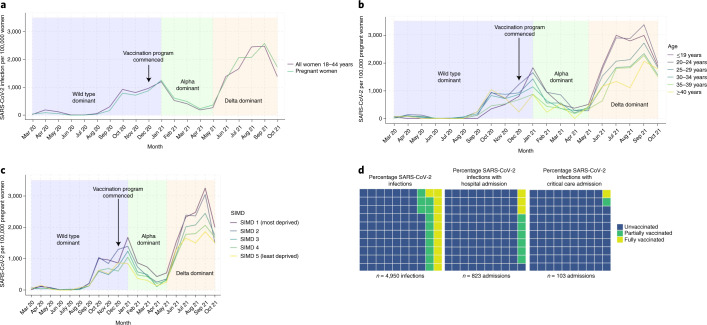
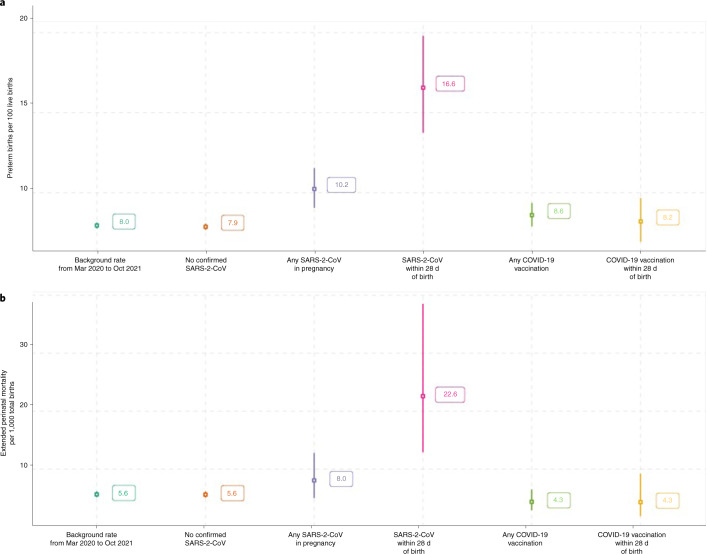
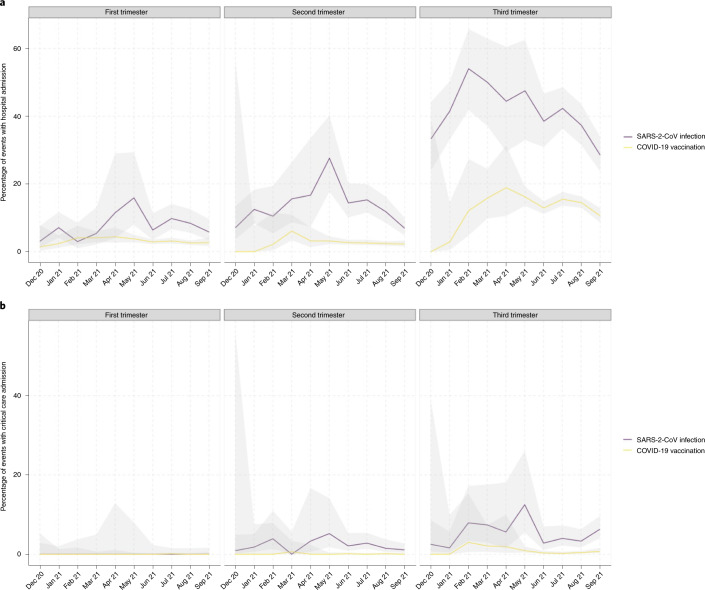
Population-level data on COVID-19 vaccine uptake in pregnancy and SARS-CoV-2 infection outcomes are lacking. We describe COVID-19 vaccine uptake and SARS-CoV-2 infection in pregnant women in Scotland, using whole-population data from a national, prospective cohort. Between the start of a COVID-19 vaccine program in Scotland, on 8 December 2020 and 31 October 2021, 25,917 COVID-19 vaccinations were given to 18,457 pregnant women. Vaccine coverage was substantially lower in pregnant women than in the general female population of 18-44 years; 32.3% of women giving birth in October 2021 had two doses of vaccine compared to 77.4% in all women. The extended perinatal mortality rate for women who gave birth within 28 d of a COVID-19 diagnosis was 22.6 per 1,000 births (95% CI 12.9-38.5; pandemic background rate 5.6 per 1,000 births; 452 out of 80,456; 95% CI 5.1-6.2). Overall, 77.4% (3,833 out of 4,950; 95% CI 76.2-78.6) of SARS-CoV-2 infections, 90.9% (748 out of 823; 95% CI 88.7-92.7) of SARS-CoV-2 associated with hospital admission and 98% (102 out of 104; 95% CI 92.5-99.7) of SARS-CoV-2 associated with critical care admission, as well as all baby deaths, occurred in pregnant women who were unvaccinated at the time of COVID-19 diagnosis. Addressing low vaccine uptake rates in pregnant women is imperative to protect the health of women and babies in the ongoing pandemic.
© 2022. The Author(s).
Conflict of interest statement
A.S. and C.R. are members of the Scottish Government’s COVID-19 Advisory Group. A.S. and C.R. are members of the New and Emerging Respiratory Virus Threats Advisory Group risk stratification subgroup. C.R. is a member of the Scientific Pandemic Influenza Group on Modeling. A.S. is a member of AstraZeneca’s Thrombotic Thrombocytopenic Advisory Group. All roles are unremunerated. R.W. and C.R. are employed by Public Health Scotland. S.J.S. has received research grants paid to the institution from Wellcome Trust, Scottish Chief Scientist Office, National Institute of Healthcare Research and Tommy’s during the course of this study. The remaining authors declare no competing interests.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
