

Identifying and predicting severe bronchiolitis profiles at high risk for developing asthma: Analysis of three prospective cohorts
- PMID: 35028545
- PMCID: PMC8741473
- DOI: 10.1016/j.eclinm.2021.101257
Identifying and predicting severe bronchiolitis profiles at high risk for developing asthma: Analysis of three prospective cohorts
Abstract
Background: Bronchiolitis is the leading cause of infants hospitalization in the U.S. and Europe. Additionally, bronchiolitis is a major risk factor for the development of childhood asthma. Growing evidence suggests heterogeneity within bronchiolitis. We sought to identify distinct, reproducible bronchiolitis subgroups (profiles) and to develop a decision rule accurately predicting the profile at the highest risk for developing asthma.
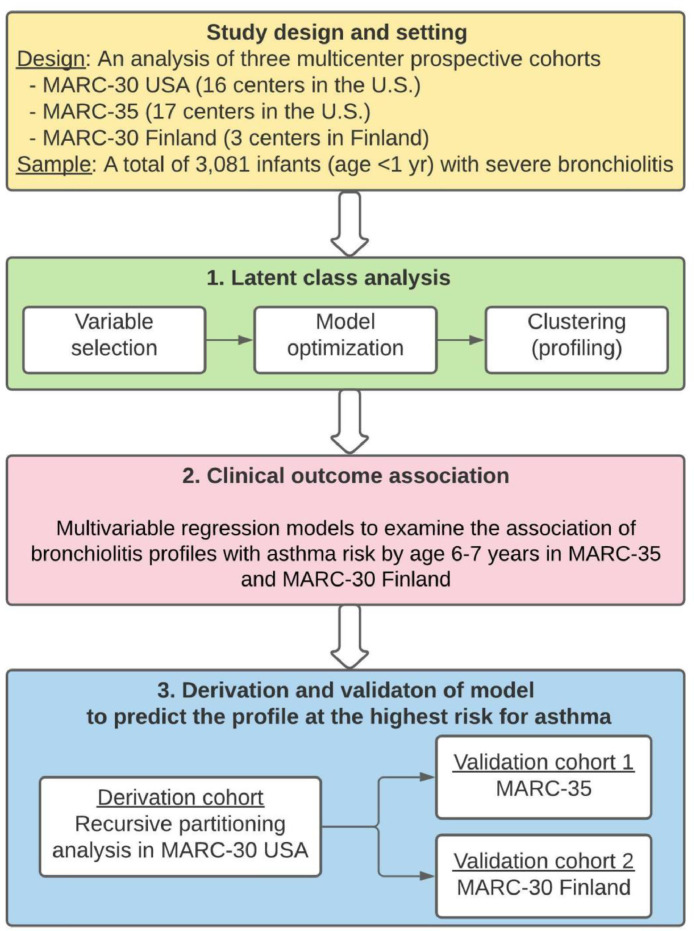
Methods: In three multicenter prospective cohorts of infants (age < 12 months) hospitalized for bronchiolitis in the U.S. and Finland (combined n = 3081) in 2007-2014, we identified clinically distinct bronchiolitis profiles by using latent class analysis. We examined the association of the profiles with the risk for developing asthma by age 6-7 years. By performing recursive partitioning analyses, we developed a decision rule predicting the profile at highest risk for asthma, and measured its predictive performance in two separate cohorts.
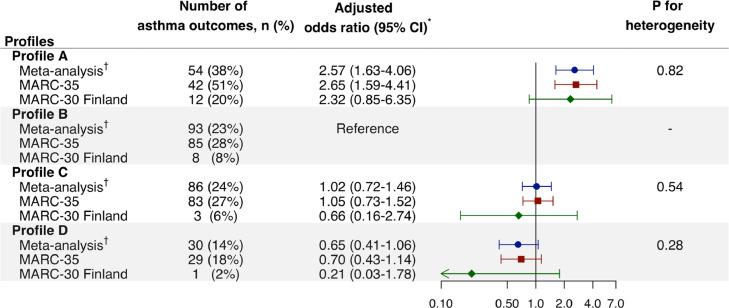
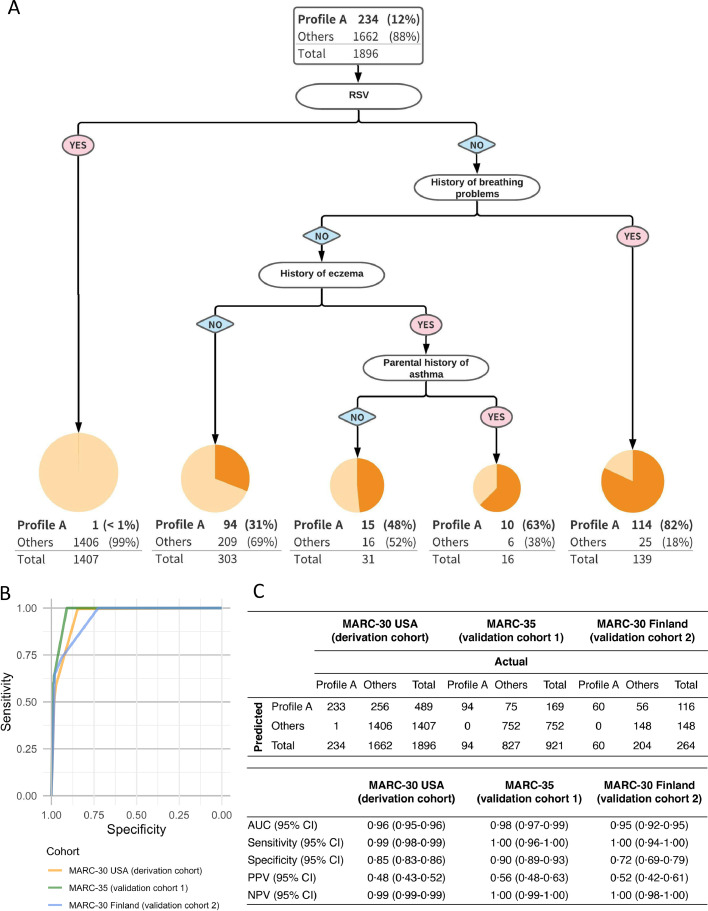
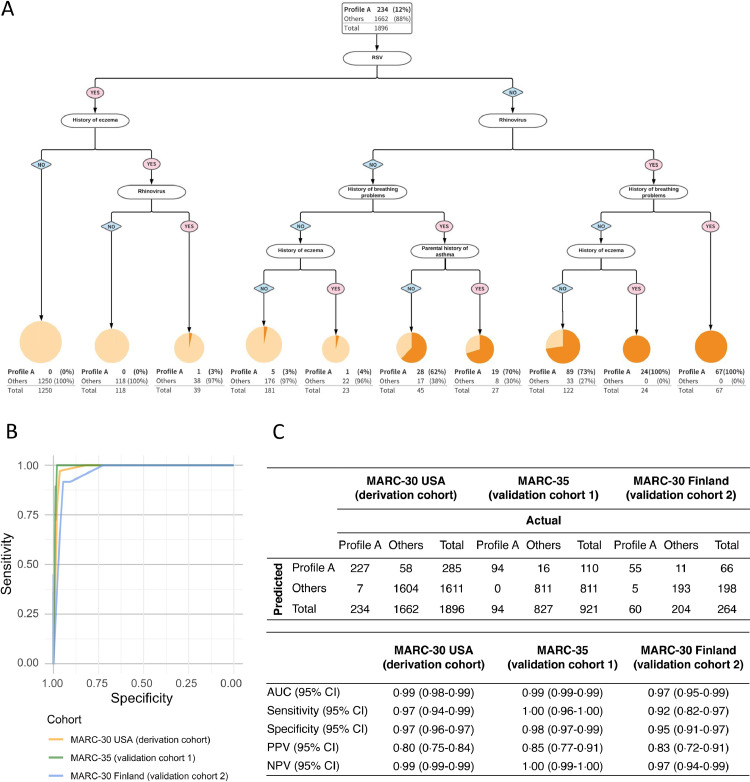
Findings: We identified four bronchiolitis profiles (profiles A-D). Profile A (n = 388; 13%) was characterized by a history of breathing problems/eczema and non-respiratory syncytial virus (non-RSV) infection. In contrast, profile B (n = 1064; 34%) resembled classic RSV-induced bronchiolitis. Profile C (n = 993; 32%) was comprised of the most severely ill group. Profile D (n = 636; 21%) was the least-ill group. Profile A infants had a significantly higher risk for asthma, compared to profile B infants (38% vs. 23%, adjusted odds ratio [adjOR] 2⋅57, 95%confidence interval [CI] 1⋅63-4⋅06). The derived 4-predictor (RSV infection, history of breathing problems, history of eczema, and parental history of asthma) decision rule strongly predicted profile A-e.g., area under the curve [AUC] of 0⋅98 (95%CI 0⋅97-0⋅99), sensitivity of 1⋅00 (95%CI 0⋅96-1⋅00), and specificity of 0⋅90 (95%CI 0⋅89-0⋅93) in a validation cohort.
Interpretation: In three prospective cohorts of infants with bronchiolitis, we identified clinically distinct profiles and their longitudinal relationship with asthma risk. We also derived and validated an accurate prediction rule to determine the profile at highest risk. The current results should advance research into the development of profile-specific preventive strategies for asthma.
Keywords: asthma; bronchiolitis; latent class analysis; phenotypes; prediction; virus.
© 2021 The Authors.
Conflict of interest statement
Kohei Hasegawa and Carlos A. Camargo, Jr. reports NIH research grants to Massachusetts General Hospital (U01 AI-067693, U01 AI-087881, R01 AI-127507, R01 AI-134940, and R01 AI-137091, and UG3/UH3 OD-023253). The other authors have no financial relationships relevant to this article to disclose.
Figures
References
-
- Régnier S.A., Huels J. Association between respiratory syncytial virus hospitalizations in infants and respiratory sequelae: systematic review and meta-analysis. Pediatr Infect Dis J. 2013;32:820–826. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
