

Insulin expression and C-peptide in type 1 diabetes subjects implanted with stem cell-derived pancreatic endoderm cells in an encapsulation device
- PMID: 35028608
- PMCID: PMC8714853
- DOI: 10.1016/j.xcrm.2021.100466
Insulin expression and C-peptide in type 1 diabetes subjects implanted with stem cell-derived pancreatic endoderm cells in an encapsulation device
Abstract
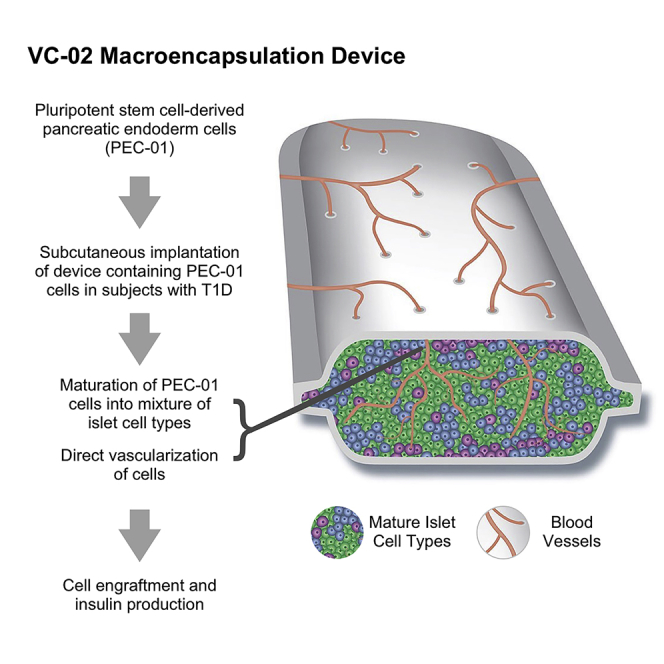
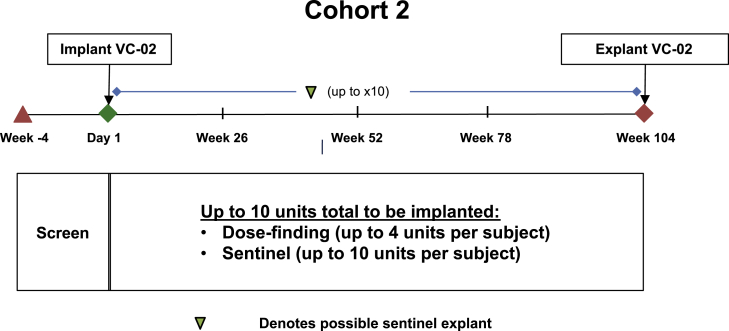
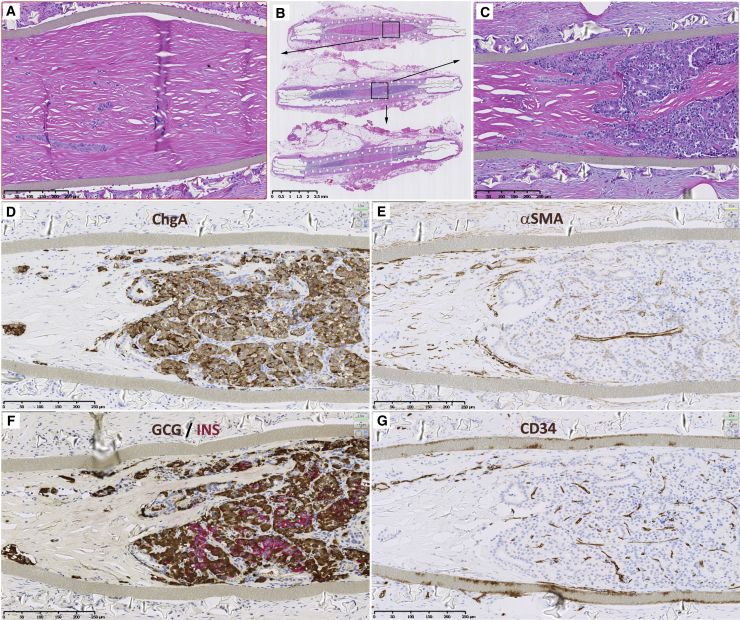
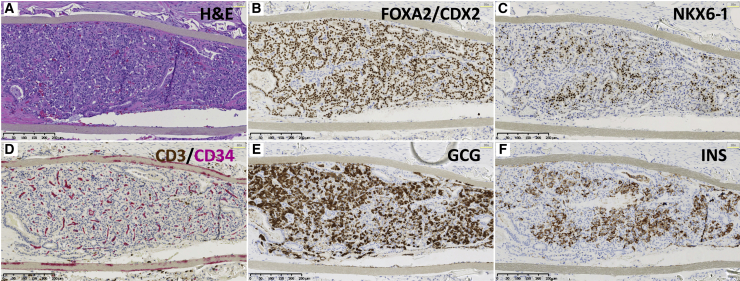
These preliminary data from an ongoing first-in-human phase 1/2, open-label study provide proof-of-concept that pluripotent stem cell-derived pancreatic endoderm cells (PEC-01) engrafted in type 1 diabetes patients become islet cells releasing insulin in a physiologically regulated fashion. In this study of 17 subjects aged 22-57 with type 1 diabetes, PEC-01 cells were implanted subcutaneously in VC-02 macroencapsulation devices, allowing for direct vascularization of the cells. Engraftment and insulin expression were observed in 63% of VC-02 units explanted from subjects at 3-12 months post-implant. Six of 17 subjects (35.3%) demonstrated positive C-peptide as early as 6 months post-implant. Most reported adverse events were related to surgical implant or explant procedures (27.9%) or to side-effects of immunosuppression (33.7%). Initial data suggest that pluripotent stem cells, which can be propagated to the desired biomass and differentiated into pancreatic islet-like tissue, may offer a scalable, renewable alternative to pancreatic islet transplants.
Trial registration: ClinicalTrials.gov NCT03163511.
© 2021 The Authors.
Conflict of interest statement
M.D., R.M.W., E.J.K., E.P.B., K.A.D., M.J., and H.L.F. are employees of ViaCyte and may have equity interest in ViaCyte, Inc., a privately held company. J.S. and J.W. are consultants for ViaCyte and may have equity interest in ViaCyte. ViaCyte has 850 global and US patents. The remaining authors declare no conflicts of interest. Funding sources for this work included the California Institute for Regenerative Medicine, JDRF, and the Stem Cell Network of Canada. These groups were not involved in the research, the writing, or the decision to submit the manuscript for publication. Authors have not been paid by a pharmaceutical company or other organization to write this article.
Figures

Comment in
-
Stem-cell derived pancreatic endoderm cells in the treatment of T1DM.Nat Rev Endocrinol. 2022 Feb;18(2):67. doi: 10.1038/s41574-021-00620-z. Nat Rev Endocrinol. 2022. PMID: 34893786 No abstract available.
-
From the dish to humans: A stem cell recipe for success.Cell Metab. 2022 Feb 1;34(2):193-196. doi: 10.1016/j.cmet.2022.01.002. Cell Metab. 2022. PMID: 35108510 Free PMC article.
References
-
- Shapiro A.M., Lakey J.R., Ryan E.A., Korbutt G.S., Toth E., Warnock G.L., Kneteman N.M., Rajotte R.V. Islet transplantation in seven patients with type 1 diabetes mellitus using a glucocorticoid-free immunosuppressive regimen. N. Engl. J. Med. 2000;343:230–238. - PubMed
-
- Hering B.J., Clarke W.R., Bridges N.D., Eggerman T.L., Alejandro R., Bellin M.D., Chaloner K., Czarniecki C.W., Goldstein J.S., Hunsicker L.G., et al. Clinical Islet Transplantation Consortium Phase 3 Trial of Transplantation of Human Islets in Type 1 Diabetes Complicated by Severe Hypoglycemia. Diabetes Care. 2016;39:1230–1240. - PMC - PubMed
-
- Lablanche S., Vantyghem M.C., Kessler L., Wojtusciszyn A., Borot S., Thivolet C., Girerd S., Bosco D., Bosson J.L., Colin C., et al. TRIMECO trial investigators Islet transplantation versus insulin therapy in patients with type 1 diabetes with severe hypoglycaemia or poorly controlled glycaemia after kidney transplantation (TRIMECO): a multicentre, randomised controlled trial. Lancet Diabetes Endocrinol. 2018;6:527–537. - PubMed
-
- Thomson J.A., Itskovitz-Eldor J., Shapiro S.S., Waknitz M.A., Swiergiel J.J., Marshall V.S., Jones J.M. Embryonic stem cell lines derived from human blastocysts. Science. 1998;282:1145–1147. - PubMed
-
- D’Amour K.A., Agulnick A.D., Eliazer S., Kelly O.G., Kroon E., Baetge E.E. Efficient differentiation of human embryonic stem cells to definitive endoderm. Nat. Biotechnol. 2005;23:1534–1541. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
