

Pulmonary Arteriovenous Malformation and Its Vascular Mimickers
- PMID: 35029077
- PMCID: PMC8814702
- DOI: 10.3348/kjr.2021.0417
Pulmonary Arteriovenous Malformation and Its Vascular Mimickers
Abstract
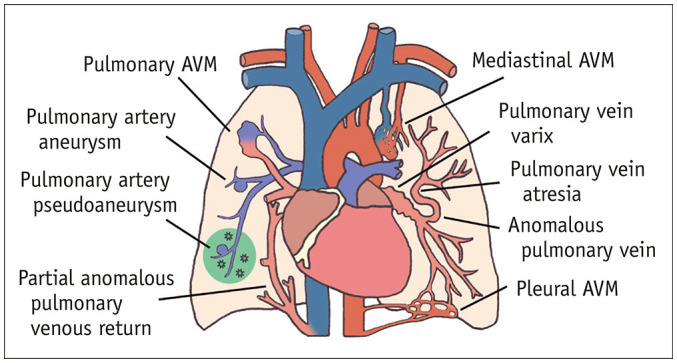
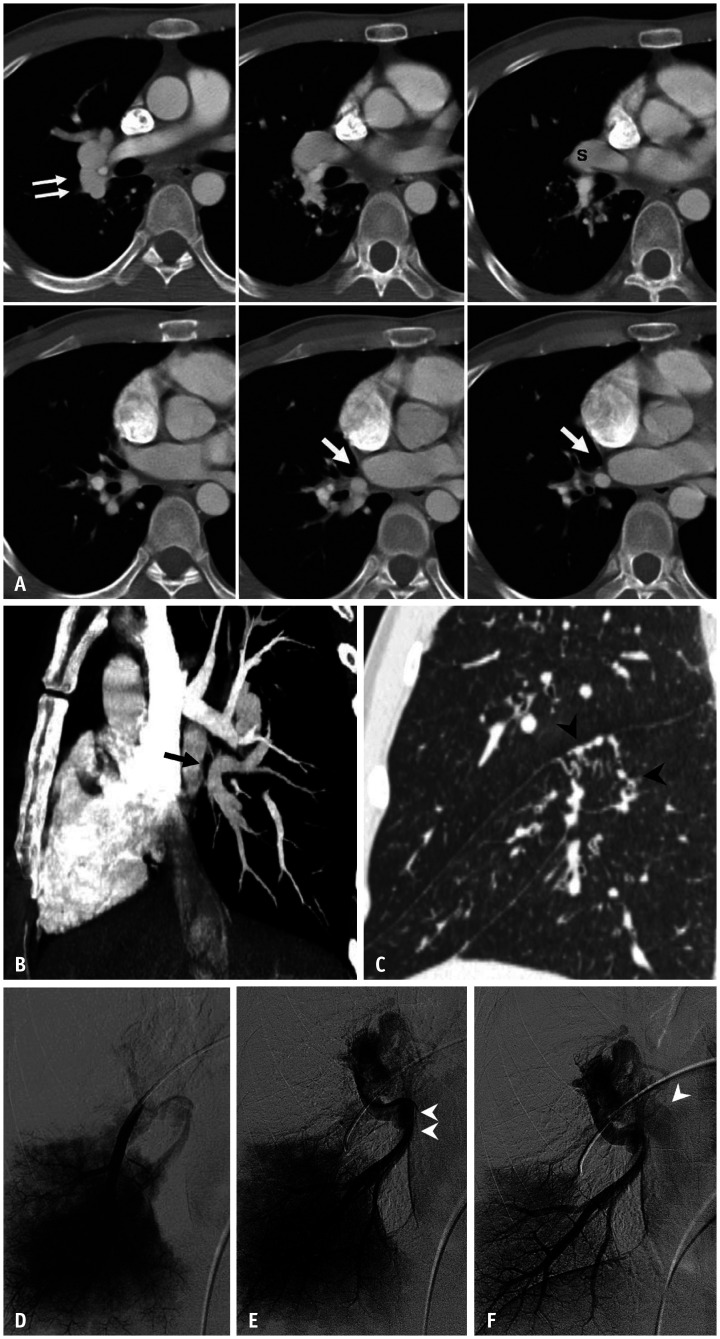
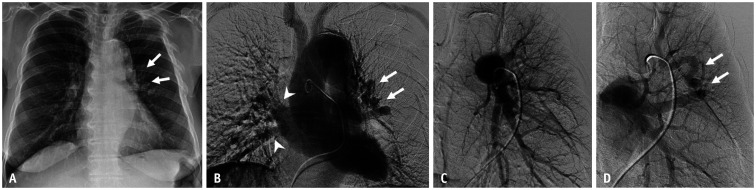
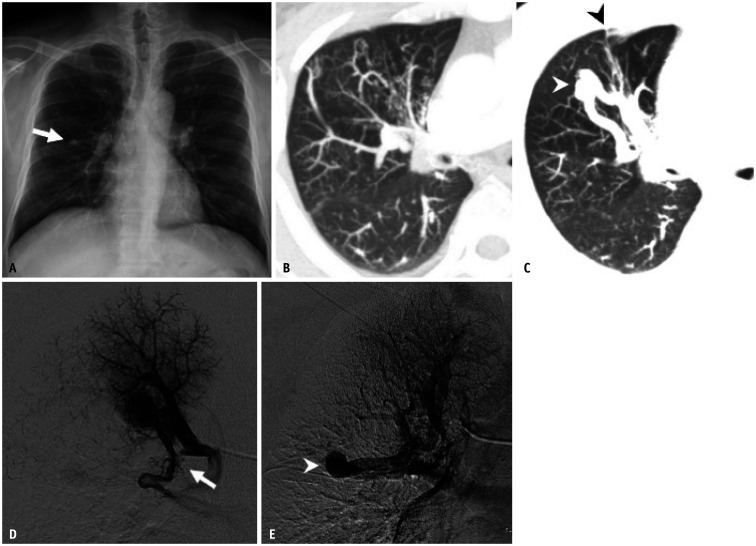
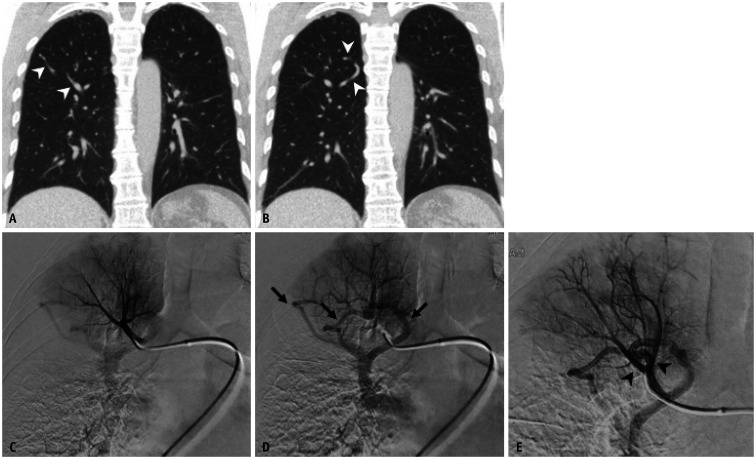
Pulmonary arteriovenous malformation (AVM) is a congenital vascular disease in which interventional radiologists can play both diagnostic and therapeutic roles in patient management. The diagnosis of pulmonary AVM is simple and can usually be made based on CT images. Endovascular treatment, that is, selective embolization of the pulmonary artery feeding the nidus of the pulmonary AVM, and/or selectively either the nidus or draining vein, has become a first-line treatment with advances in interventional devices. However, some vascular diseases can simulate pulmonary AVMs on CT and pulmonary angiography. This subset can confuse interventional radiologists and referring physicians. Vascular mimickers of pulmonary AVM have not been widely known and described in detail in the literature, although some of these require surgical correction, while others require regular follow-up. This article reviews the clinical and radiologic features of pulmonary AVMs and their mimickers.
Keywords: Aneurysm; Arteriovenous malformations; Diagnosis, differential; Lung; Pleura; Scimitar syndrome; Stenosis, pulmonary vein; Thoracic wall.
Copyright © 2022 The Korean Society of Radiology.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
References
-
- Hanson JM, Wood AM, Seymour R, Petheram IS. Anomalous unilateral single pulmonary vein: two cases mimicking arteriovenous malformations and a review of the literature. Australas Radiol. 2005;49:246–251. - PubMed
-
- Tokunaga K, Kubo T, Yamaoka T, Isoda H, Togashi K. Can the “pine-needle sign” on computed tomography be used to differentiate pulmonary arteriovenous malformation from its mimics? Analysis based on dynamic contrast-enhanced chest computed tomography in adults. Eur J Radiol. 2017;95:314–318. - PubMed
-
- Gill SS, Roddie ME, Shovlin CL, Jackson JE. Pulmonary arteriovenous malformations and their mimics. Clin Radiol. 2015;70:96–110. - PubMed
-
- Hyun D, Do YS, Lim SJ, Park HS, Park KB. Anomalous unilateral single pulmonary vein mimicking pulmonary arteriovenous malformation. Cardiovasc Intervent Radiol. 2014;37:835–838. - PubMed
-
- Lin CT, Zimmerman SL, Mitchell SE, Fishman EK. Pulmonary venous anomalies causing misdiagnosis of pulmonary arteriovenous malformations. Clin Imaging. 2018;47:96–100. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
