

Predicting Risk of Surgery in Patients With Small Bowel Crohn's Disease Strictures Using Computed Tomography and Magnetic Resonance Enterography
- PMID: 35032168
- PMCID: PMC9924041
- DOI: 10.1093/ibd/izab332
Predicting Risk of Surgery in Patients With Small Bowel Crohn's Disease Strictures Using Computed Tomography and Magnetic Resonance Enterography
Abstract
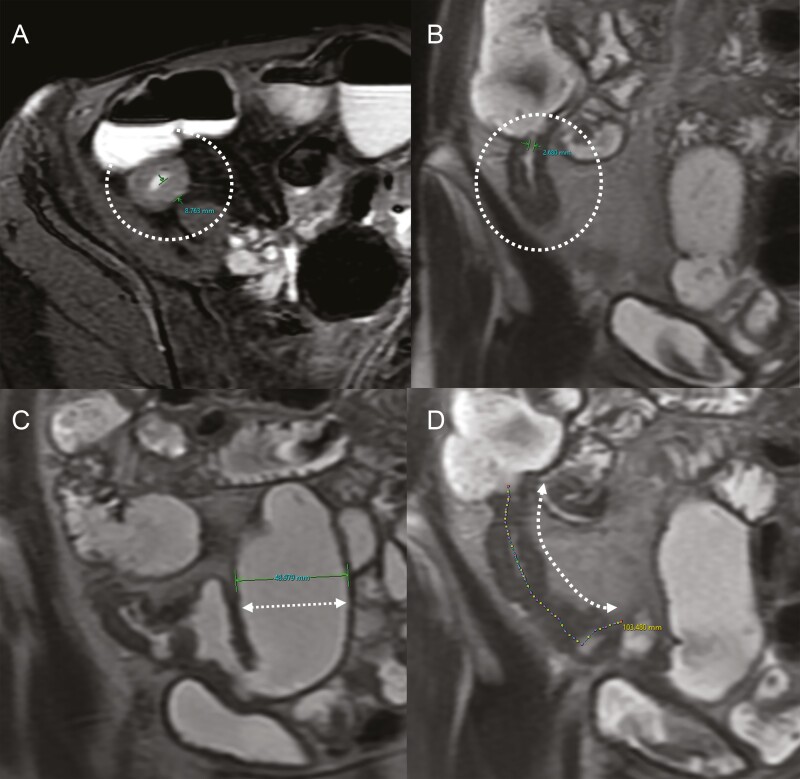
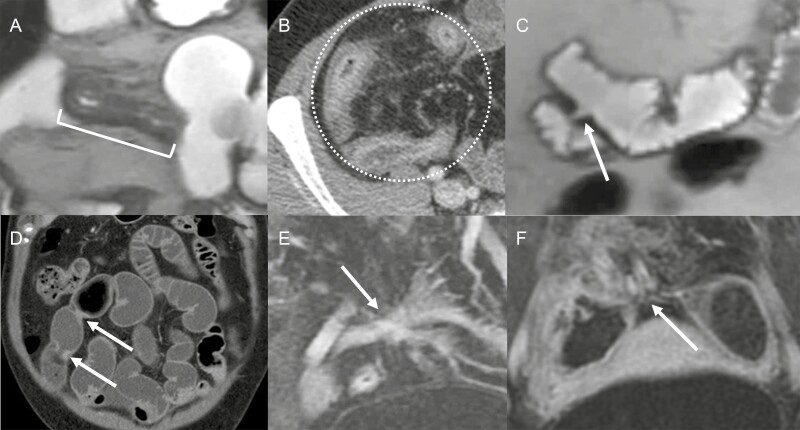
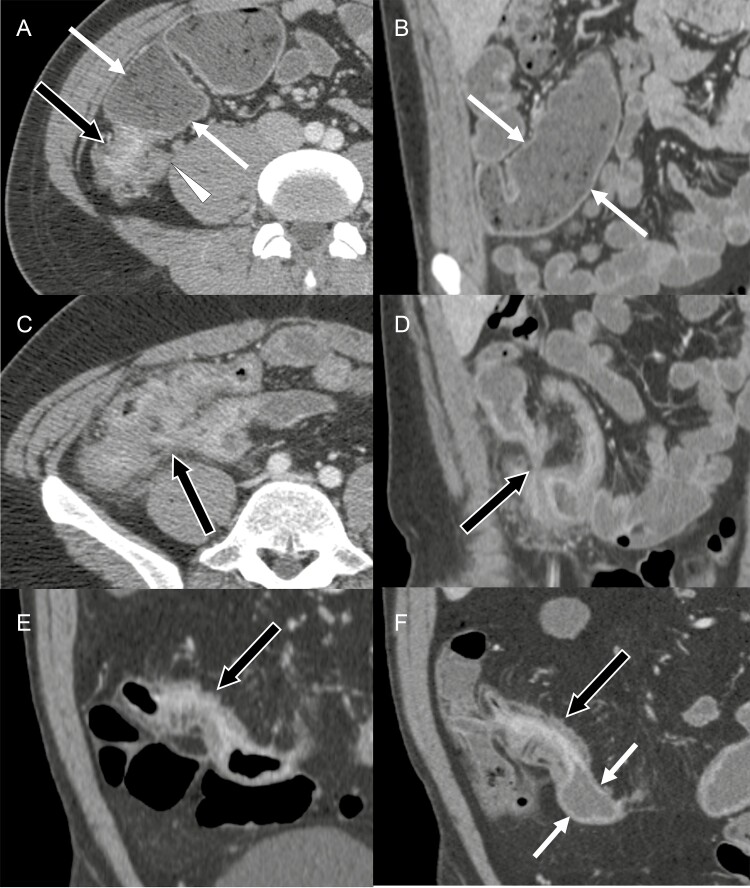
Background: We aimed to determine if patient symptoms and computed tomography enterography (CTE) and magnetic resonance enterography (MRE) imaging findings can be used to predict near-term risk of surgery in patients with small bowel Crohn's disease (CD).
Methods: CD patients with small bowel strictures undergoing serial CTE or MRE were retrospectively identified. Strictures were defined by luminal narrowing, bowel wall thickening, and unequivocal proximal small bowel dilation. Harvey-Bradshaw index (HBI) was recorded. Stricture observations and measurements were performed on baseline CTE or MRE and compared to with prior and subsequent scans. Patients were divided into those who underwent surgery within 2 years and those who did not. LASSO (least absolute shrinkage and selection operator) regression models were trained and validated using 5-fold cross-validation.
Results: Eighty-five patients (43.7 ± 15.3 years of age at baseline scan, majority male [57.6%]) had 137 small bowel strictures. Surgery was performed in 26 patients within 2 years from baseline CTE or MRE. In univariate analysis of patients with prior exams, development of stricture on the baseline exam was associated with near-term surgery (P = .006). A mathematical model using baseline features predicting surgery within 2 years included an HBI of 5 to 7 (odds ratio [OR], 1.7 × 105; P = .057), an HBI of 8 to 16 (OR, 3.1 × 105; P = .054), anastomotic stricture (OR, 0.002; P = .091), bowel wall thickness (OR, 4.7; P = .064), penetrating behavior (OR, 3.1 × 103; P = .096), and newly developed stricture (OR: 7.2 × 107; P = .062). This model demonstrated sensitivity of 67% and specificity of 73% (area under the curve, 0.62).
Conclusions: CTE or MRE imaging findings in combination with HBI can potentially predict which patients will require surgery within 2 years.
Keywords: Crohn disease; computed tomography enterography; magnetic resonance enterography; predictive model; surgical intervention.
Plain language summary
Computed tomography and magnetic resonance enterography imaging measurements and observations, in combination with patient symptoms, can potentially predict which patients will require surgery within 2 years with modest degree of accuracy.
© The Author(s) 2022. Published by Oxford University Press on behalf of Crohn’s & Colitis Foundation. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Cosnes J, Cattan S, Blain A, et al. . Long-term evolution of disease behavior of Crohn’s disease. Inflamm Bowel Dis. 2002;8:244-250. - PubMed
-
- Torres J, Mehandru S, Colombel JF, Peyrin-Biroulet L. Crohn’s disease. Lancet. 2017;389:1741-1755. - PubMed
-
- Peyrin-Biroulet L, Loftus EV Jr, Colombel JF, Sandborn WJ. The natural history of adult Crohn’s disease in population-based cohorts. Am J Gastroenterol. 2010;105:289-297. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
