

Prediction and risk stratification from hospital discharge records based on Hierarchical sLDA
- PMID: 35033059
- PMCID: PMC8760773
- DOI: 10.1186/s12911-022-01747-3
Prediction and risk stratification from hospital discharge records based on Hierarchical sLDA
Abstract
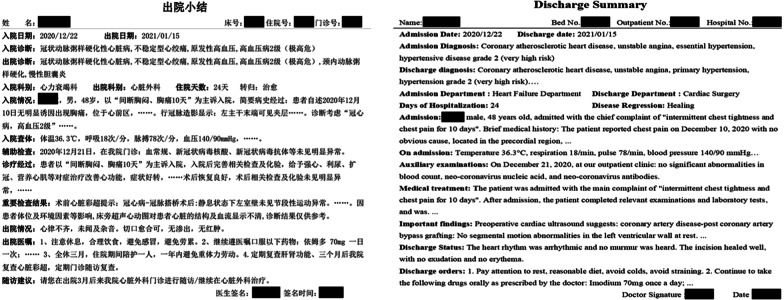
Background: The greatly accelerated development of information technology has conveniently provided adoption for risk stratification, which means more beneficial for both patients and clinicians. Risk stratification offers accurate individualized prevention and therapeutic decision making etc. Hospital discharge records (HDRs) routinely include accurate conclusions of diagnoses of the patients. For this reason, in this paper, we propose an improved model for risk stratification in a supervised fashion by exploring HDRs about coronary heart disease (CHD).
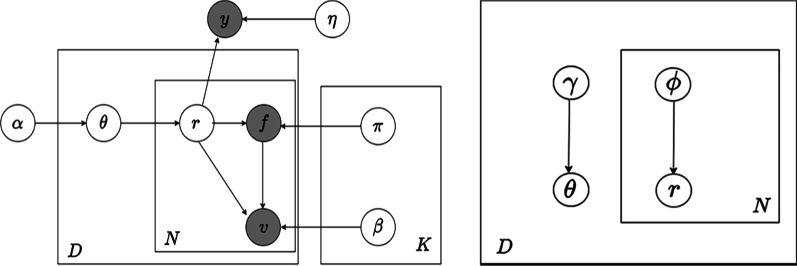
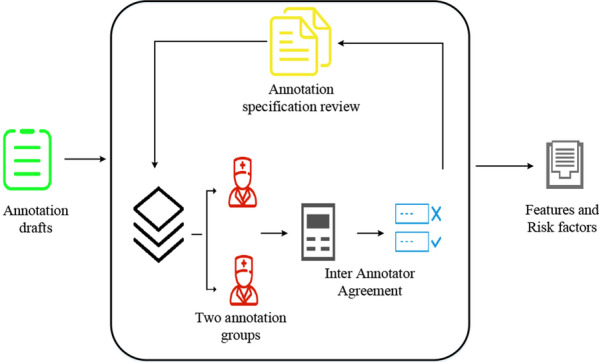
Methods: We introduced an improved four-layer supervised latent Dirichlet allocation (sLDA) approach called Hierarchical sLDA model, which categorized patient features in HDRs as patient feature-value pairs in one-hot way according to clinical guidelines for lab test of CHD. To address the data missing and imbalance problem, RFs and SMOTE methods are used respectively. After TF-IDF processing of datasets, variational Bayes expectation-maximization method and generalized linear model were used to recognize the latent clinical state of a patient, i.e., risk stratification, as well as to predict CHD. Accuracy, macro-F1, training and testing time performance were used to evaluate the performance of our model.
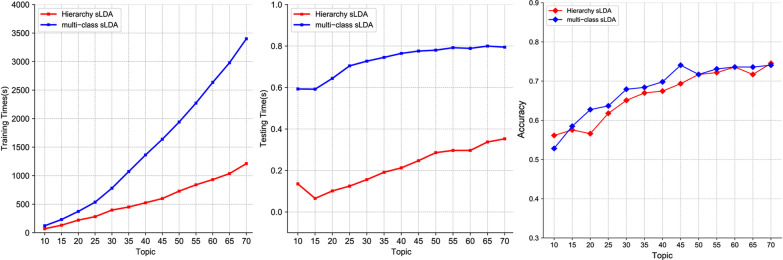
Results: According to the characteristics of our datasets, i.e., patient feature-value pairs, we construct a supervised topic model by adding one more Dirichlet distribution hyperparameter to sLDA. Compared with established supervised algorithm Multi-class sLDA model, we demonstrate that our proposed approach enhances training time by 59.74% and testing time by 25.58% but almost no loss of average prediction accuracy on our datasets.
Conclusions: A model for risk stratification and prediction of CHD based on sLDA model was proposed. Experimental results show that Hierarchical sLDA model we proposed is competitive in time performance and accuracy. Hierarchical processing of patient features can significantly improve the disadvantages of low efficiency and time-consuming Gibbs sampling of sLDA model.
Keywords: Hospital discharge records; Risk stratification; Supervised latent Dirichlet allocation; Topic models.
© 2022. The Author(s).
Conflict of interest statement
The authors report that they have no conflicts.
Figures

References
-
- Schlesinger DE, Stultz CM. Deep learning for cardiovascular risk stratification. Curr Treat Options Cardiovasc Med. 2020 doi: 10.1007/s11936-020-00814-0. - DOI
-
- Matheny M, Mcpheeters ML, et al. Systematic review of cardiovascular disease risk assessment tools [Internet] Rockville (MD): Agency for Healthcare Research and Quality (US); 2011. - PubMed
-
- Hsueh PYS, Zhu XX, et al. Automatic summarization of risk factors preceding disease progression an insight-driven healthcare service case study on using medical records of diabetic patients. World Wide Web Internet Web Inf Syst. 2015;18(4):1163–1175. doi: 10.1007/s11280-014-0304-2. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
